Mice have been increasingly used to study kidney disease, not only because of their small size and homology with humans, but also because of the ability to manipulate genes by knockdown, knockout, and over expression systems. Scientists have produced a variety of inbred strains with varying degrees of susceptibility to kidney injury. Over the last several decades, the development of multiple kidney fibrosis models has allowed for sophisticated study of fibrotic pathways that ultimately has led to not only a better understanding of fibrosis, but also a model in which potential therapeutic agents can be tested. For example, if we knockout gene X and then induce kidney fibrosis, the resulting kidney pathology may provide some insight into gene X’s role in kidney fibrosis. The most robust studies use a combination of the models below and it is important not to rely on only one model.
Let’s review some of the most popular models of fibrosis:
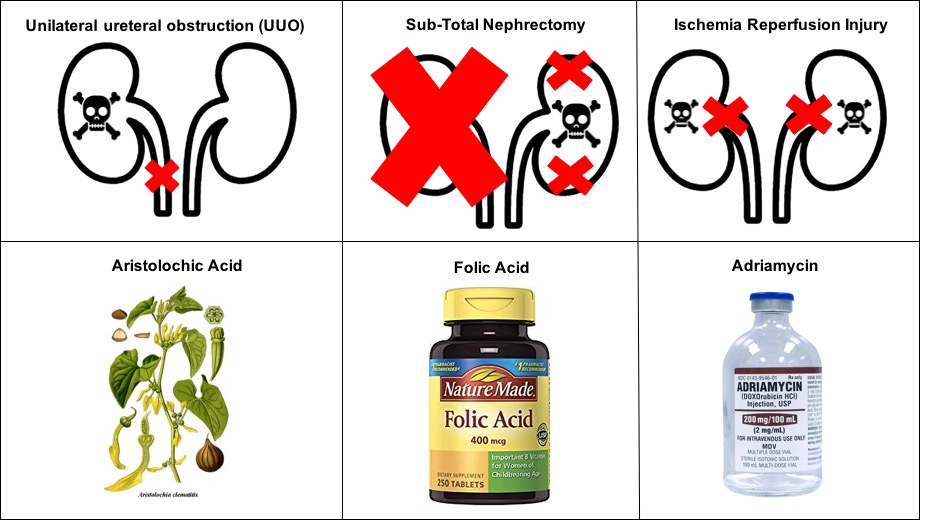
1. Unilateral ureteral obstruction (better known as “UUO”): As the name implies, the UUO model involves physically tying off one of the ureters with a suture which leads to interstitial fibrosis due to both hemodynamic and metabolic changes. This model has been used since the 1970s in a wide variety of animals: first in lambs, and later possums, rabbits, pigs, dogs, monkeys, rats, and mice. The obstruction leads to tubular injury and cell death by apoptosis and necrosis, glomerulopathy, infiltration of macrophages and cytokine release, proliferation of fibroblasts, and eventually severe fibrosis seven days after the obstruction in wild type mice. The surgery is relatively easy to perform and can be completed in 15 – 20 minutes. While the contralateral kidney can serve as the control kidney in UUO experiments, it also compensates for the injured kidney and thus markers of kidney function such as serum creatinine and urea provide limited information. While this is a convenient model to induce fibrosis, many have argued that the mechanism of fibrosis in UUO is rapid and extensive and thus might not be reflective of human CKD. However, UUO remains one of the most popular methods.
2. Sub-Total Nephrectomy: Like the name implies, this is surgical removal of just about all kidney parenchyma. To achieve this, unilateral nephrectomy is first performed followed by either ligation of the contralateral renal artery branches (which leads to infarction of both renal poles) or ablation and excision of 50% of the contralateral kidney. Though the ligation model cannot be performed as easily in mice due to limited renal artery branching branching, this model leads to more severe proteinuria. The remnant kidney develops both glomerulosclerosis and tubulointerstitial fibrosis. This model is most commonly performed in rats, as there can be some variability with mice depending on the strain and amount of tissue excised. Interestingly, one strain of mice carries only one copy of the renin gene and thus fibrosis phenotypes may be less severe given the pathogenic importance of the renin-angiotensin system.
3. Aristolochic-acid (AA) nephropathy: While AA-induced nephropathy commonly shows up on the nephrology board exam, intraperitoneal injection of AA into wild type mice leads to a phenotype similar to chronic tubulointerstitial fibrosis that is seen in humans. Unlike UUO, the development of fibrosis can take several weeks depending on the AA dosing and frequency of administration.
4. Adriamycin nephropathy: In 1977, a case of kidney injury due to the anthracycline Adriamycin (doxorubicin) was described. In rodents, doxorubicin also induces a phenotype similar to chronic proteinuric kidney disease with histological changes of focal segmental and global glomerulosclerosis, podocyte fusion, and tubulointerstitial inflammation and fibrosis. Changes can be seen as early as 1-2 weeks after intravenous administration and become more severe by week 4. Unlike the relative ease of UUO or intraperitoneal administration, intravenous injections in rodents can be challenging due to small vein sizes.
5. Folic acid nephropathy: The seemingly harmless water-soluble B vitamin can cause acute tubular necrosis and chronic interstitial fibrosis when administered in mice intraperitoneally at extremely high doses. Folic acid both obstructs the tubular lumen by forming crystals and is directly toxic to the tubular epithelial cells.
6. Ischemia-Reperfusion Injury (IRI): The IRI model is commonly used to study acute kidney injury (AKI), but long term outcomes include tubular atrophy, interstitial fibrosis, and inflammation. In a model of bilateral IRI, clamping of renal pedicles for 21 minutes led to significantly elevated levels of serum creatine and urea at 1 year. Histology at one year revealed significant scarring and immune infiltration. Though the development of fibrosis here requires a longer period of time, the IRI model closely mimics IRI experienced by deceased donor kidney transplants.
In addition to these 6 models, numerous other models have been utilized to induce fibrosis. Share your favorite models in the comments below.
Samira Farouk, MD
NSMC Intern 2018, Chief Nephrology Fellow
Icahn School of Medicine at Mount Sinai