Recently the FDA approved one of the newer exchange resins (Lokelma, ZS-9) for the treatment of hyperkalemia. (Veltassa, Patiromer), a calcium based cation exchange resin, was recently developed and approved since 2015 for the treatment of hyperkalemia. These two new drugs, which each have large randomized placebo controlled trials confirming their effectiveness, now seem bound to replace the ancient but much experienced Kayexalate (Sodium Polystyrene Sulfonate; SPS) for the management of hyperkalemia. However, they are not approved in Canada and their cost makes them less enticing options in a publicly funded health care system. Also, what about safety concerns? SPS has been used since the 1950s, however it took decades for case reports to come out possibly linking fatal colon necrosis to Kayexalate use. This association remains hotly debated. A systematic review in 2013 found a total of 58 cases of biopsy confirmed bowel injury that were “possibly” related to SPS use based on the WHO causality criteria. Interestingly, these cases were not limited to patients using SPS with sorbitol, nor to the post-operative population as was once thought to be the major risk factors for adverse GI events from SPS. On the other hand, a retrospective single-centre review over a 10 year period found only 3 cases of colon necrosis among 2,194 patients having received SPS. When they compared this incidence of colon necrosis to control patients having not received SPS, they found a non-significant RR of 2.10 (0.66-6.64; P=0.2). Many nephrologists will argue that SPS has a long standing proven track record and that colon necrosis is such a rare side effect that it is unlikely to be related. While no one knows if this is truly the case, the uncertainty surrounding this issue is one of the major reasons that led to the development of the newer exchange resins: ZS-9 and patiromer.
Before praising and widely accepting these newer, expensive products, would it not be wise to use the same caution we would for SPS? It can take years for such a rare adverse event as colon necrosis to manifest itself, how do we know we won’t be facing this GI safety issue 5 to 10 years from now?
Perhaps we could look for other ways of trying to enhance GI elimination of potassium.
 |
|
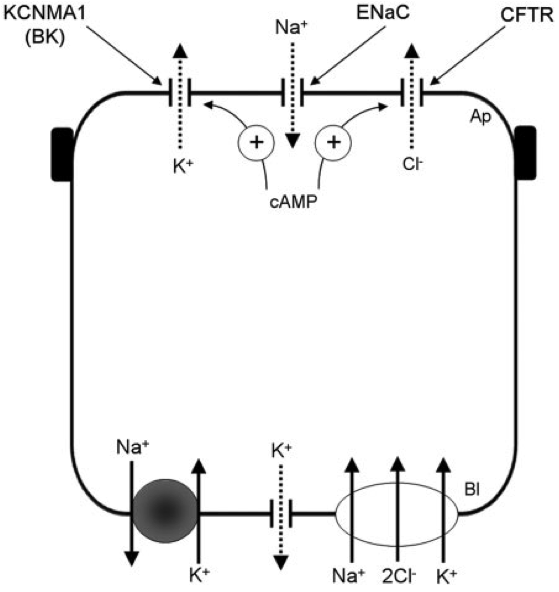
BK-channel in colon enterocyte (Source: Sandle et al. QJM. 2010 Feb;103(2):85-9)
The colonic enterocyte has an ability to excrete potassium in stool. This may be an important physiologic property in patients with advanced CKD who lose the ability to renally excrete potassium. In fact, patients with ESKD are known to have a greater excretion of potassium in their stool compared to individuals with normal kidney function. An important transporter involved in this process is the BK-channel located on the apical side of the colonic enterocyte within the colon crypts (see Figure). This channel is responsible for actively secreting potassium in the GI lumen. Aldosterone stimulates this channel, enhancing K secretion in the stool, similar to its effect in the kidneys. In fact, a study in the 1970s of patients suffering from acute cholera showed that within 12 hours of receiving a single dose of 100mg of spironolactone, there was a significant decrease in stool loss of potassium and an increase in stool loss of sodium. This likely is a major reason explaining why anuric patients with ESKD may still have from hyperkalemia if given RAAS blockade. The BK channel will also be stimulated by various diarrheal states such as Ogilvie’s syndrome, villous adenoma and certain laxatives such as bisacodyl. Bisacodyl is a stimulant laxative which enhances peristalsis through parasympathetic nerve activation, but also stimulates cAMP production within the colon enterocyte. This cAMP is thought to enhance K excretion via the BK-channel. A study performed in 2005 used immunohistologic analysis of colonic enterocytes in patients with ESKD and showed that BK-channels are upregulated in these patients compared to controls with normal kidney function. The upregulation of BK-channels probably represent an adaptation to chronic potassium load in order to maintain homeostasis. Interestingly, a small study in 2003 tested the effect of Bisacodyl on potassium in patients with ESKD. Eight controls normal kidney function and 13 patients with ESKD were given Bisacodyl 5-10mg PO titrated to achieve 2 soft bowel movements per day and these were compared to 5 ESKD patients given lactulose 10ml PO titrated also to 2 soft bowel movements per day. After 2 weeks of treatment, they found that the ESKD patients with Bisacodyl had a significant decrease in potassium from 5.9 to 5.4mmol/L whereas the controls given Bisacodyl and the ESKD patients given lactulose had no change in potassium values after 2 weeks of therapy. This suggests that Bisacodyl increases potassium excretion in the stool in patients with ESKD through a mechanism not simply related to its laxative effect, but likely through stimulation of the BK-channel of the colonic enterocyte. It is unfortunate that no further studies have looked into this therapeutic option for maintaining potassium homeostasis in patients with advanced CKD. Unfortunately, we don’t know if Bisacodyl would work as well in the non-dialysis population since we could expect these patients may not have as upregulated BK channels as in ESKD who are faced with more chronically elevated potassium loads. However, this would be an interesting study to pursue since Bisacodyl would be a cheap and safe way of controlling potassium in patients with advanced CKD by enhancing the body’s natural adaptation to potassium handling.
David Massicotte-Azarniouch
Nephrology Fellow
University of Ottawa
![]() Previous Post
Previous Post
Dear Future Independent Investigator in Nephrology…
![]() Next Post
Next Post
GlomCon Nephropathology Essentials
|