The tubulointerstitium of the kidney is broadly divided into the cortex and the medulla. These are extremely important components of the kidney, which can show a broad spectrum of changes ranging from subtle to significant, in both acute and chronic kidney injury. Therefore, in order to recognize the pathologic changes in these areas, one must first be familiar with its normal architecture
In this post, we will cover the main histologic features of the normal tubulointerstitium as seen on diagnostic kidney biopsies. For a more in-depth review please refer to my favorite references for kidney pathology: Heptinstall’s Pathology of the Kidney, Silva’s Diagnostic Renal Pathology and Renal Pathophysiology, The Essentials.
Architecturally, the kidney cortex is divided into outer and inner areas, namely the cortical labyrinth and the medullary rays.
Cortical labyrinth
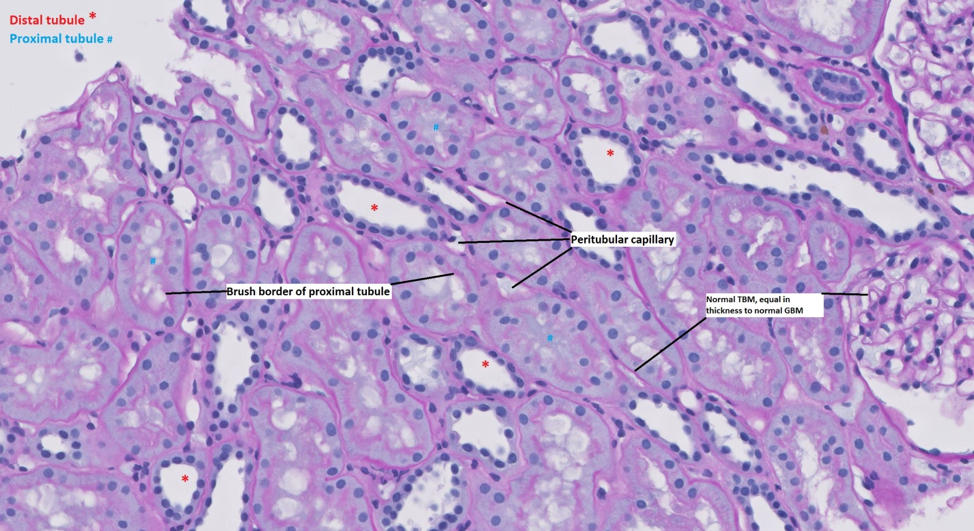
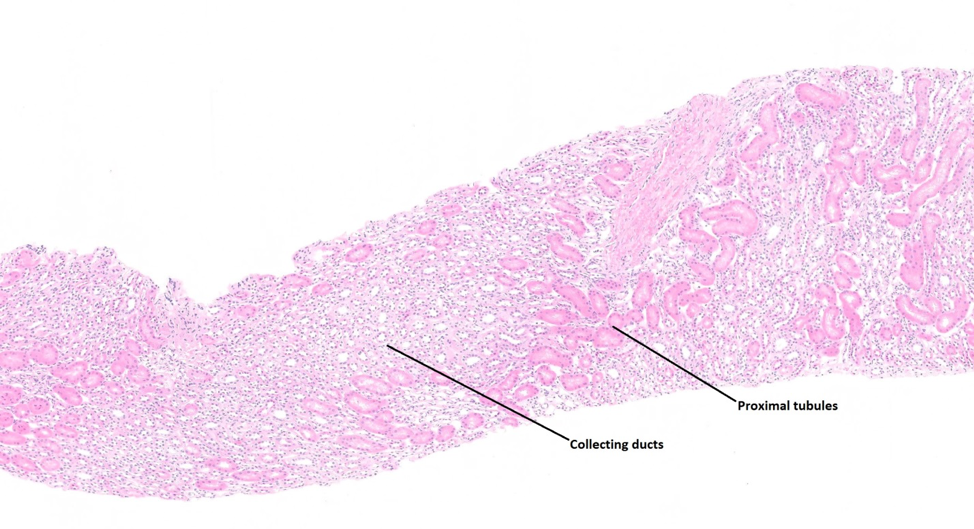
This is the most common portion of the tubulointerstitium seen in diagnostic kidney biopsies and is the outer portion of the cortex which contains glomeruli, proximal tubules, distal tubules, interlobular arteries, interlobular veins, arterioles, venules and peritubular capillaries. In a normal appearing kidney, the tubules are arranged in a back to back manner (i.e.: tubular basement membranes of adjacent tubules next to each other). The tubules are bound by a thin tubular basement membrane, which is about the same thickness as that of a normal glomerular capillary loop.
Proximal tubules contain epithelial cells with round nuclei and abundant cytoplasm. The luminal aspect of proximal tubular epithelial cells show prominent brush borders which are typically PAS positive. The brush border is a useful structure to look for when identifying normal proximal tubules, and when looking for acute tubular epithelial cell injury (one of the earliest signs of ATN is loss of the proximal tubular brush border).
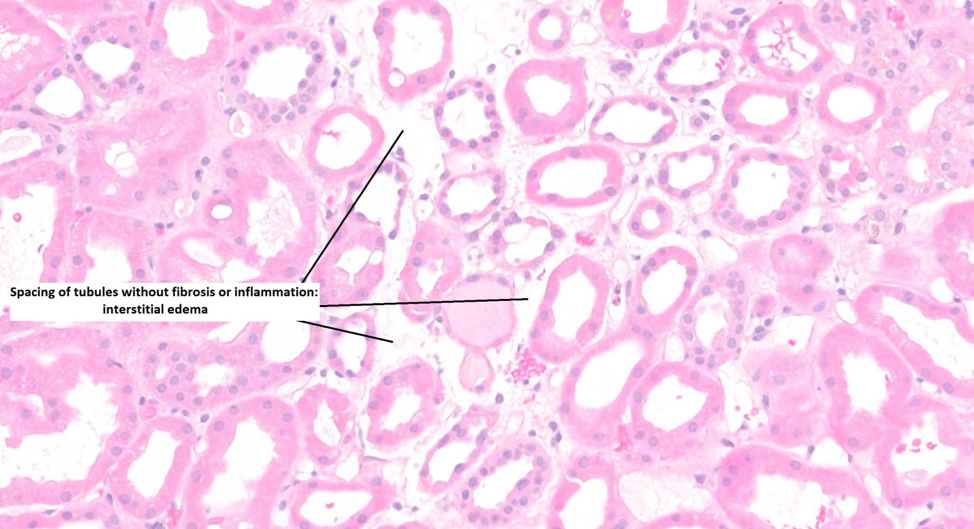
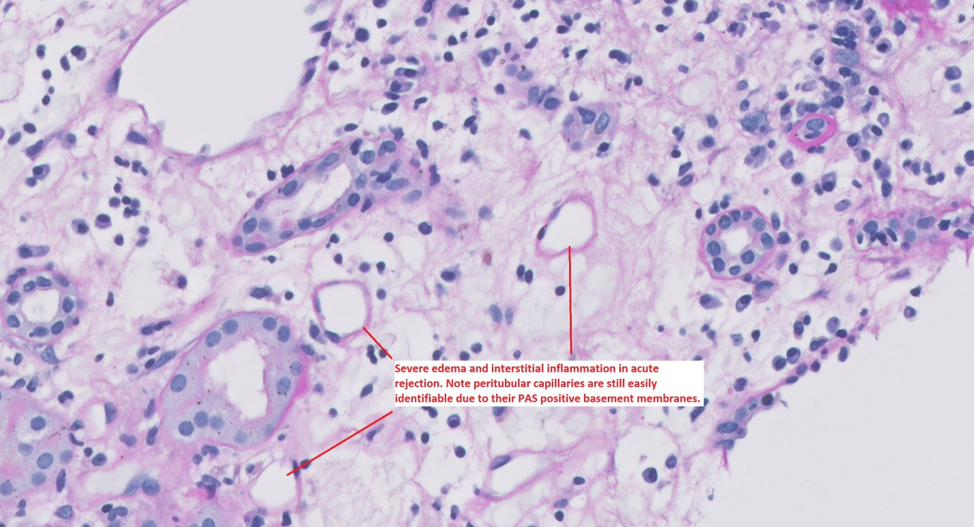
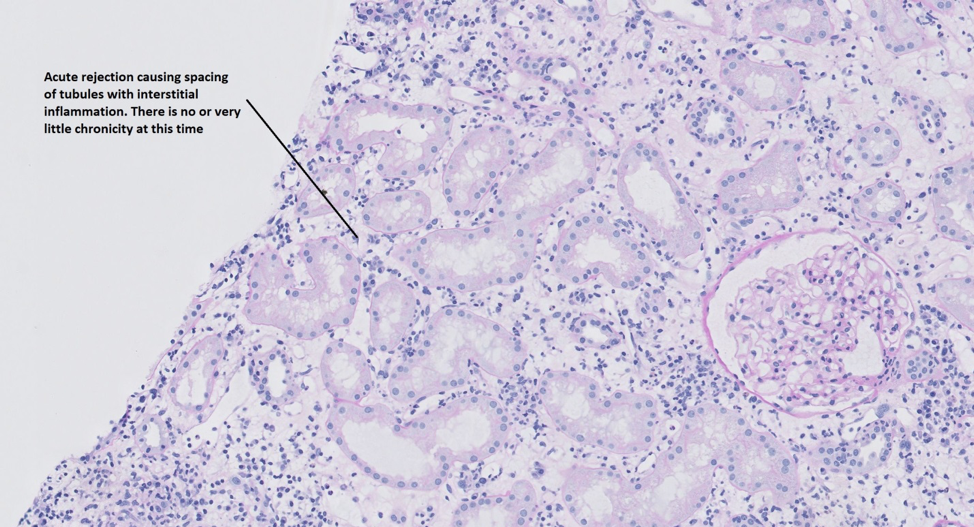
Interspersed between the proximal tubules are distal tubules which are less in number, and characterized by epithelial cells with a flatter appearance with small nuclei and scant cytoplasm. Distal tubular epithelial cells do not have brush borders. In between the proximal and distal tubules are in peritubular capillaries. These are important structures to recognize, especially in transplant biopsies when looking for peritubular capillaritis. Peritubular capillaries are often difficult to visualize on H&E stain, but are very easy to see on PAS stained sections. The PAS stain will highlight the basement membranes of the peritubular capillaries which clearly separate them from the surrounding interstitium, even when there is interstitial edema or inflammation. The interstitial space is barely visible in normal kidneys, and therefore interstitial spacing, i.e. separation of tubules, is a subtle (or obvious) clue to an underlying pathologic change.
There are 3 main diagnostic considerations for interstitial spacing which are: interstitial fibrosis, interstitial edema and interstitial inflammation.
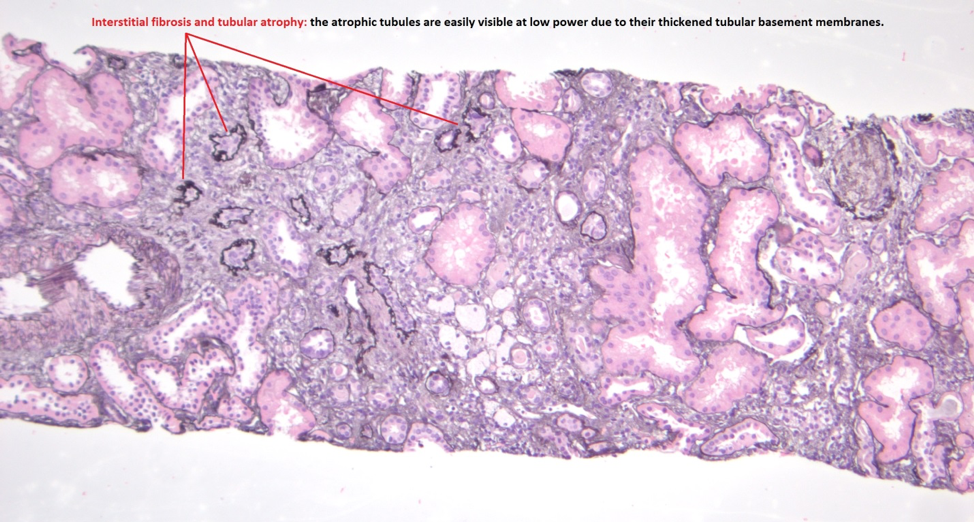
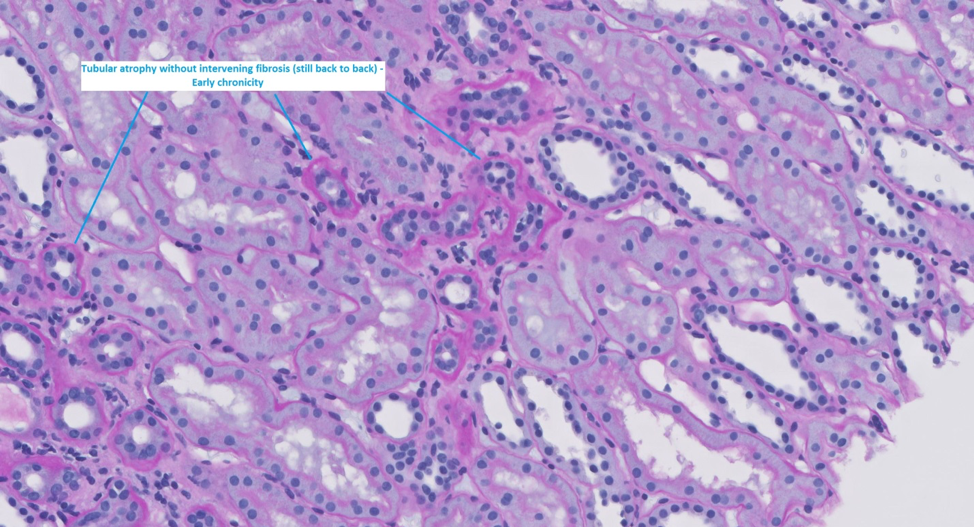
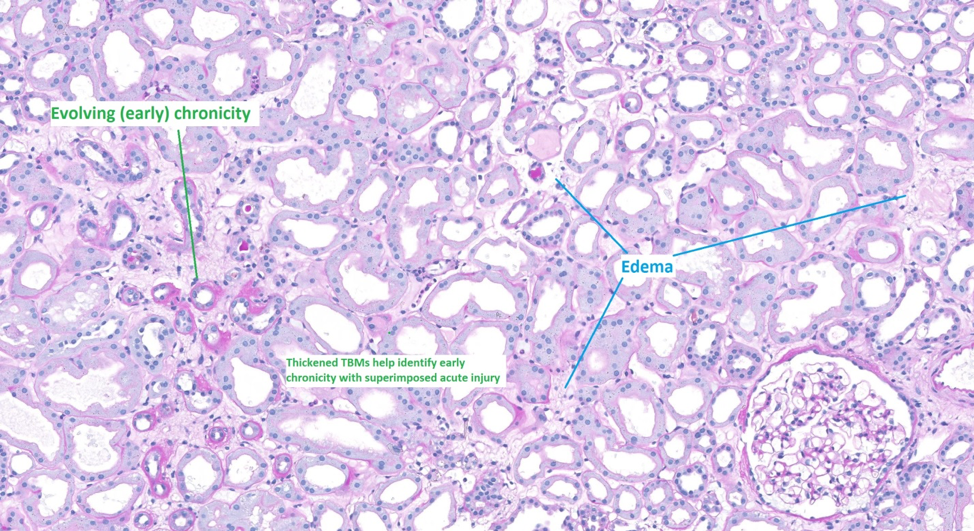
Interstitial fibrosis is defined as deposition of collagen in the interstitial space. Interstitial fibrosis is usually accompanied by tubular atrophy (although not always). Identifying tubular atrophy is often helpful when assessing for chronicity and this can be done even at low power as atrophic tubules will have thickened tubular basement membranes (most visible on PAS or Jones stain). This is particularly helpful when assessing for chronicity on biopsies with lots of inflammation or edema.
That brings us to our second reason for spacing of tubules – edema. Edema and fibrosis can sometimes be very difficult to distinguish from one another. In certain cases there can be fibrosis with superimposed edema which can be even more challenging to distinguish. Again in these cases, look for areas of tubular atrophy, and compare those areas on the trichrome stain. The trichrome will stain areas of fibrosis as a bright bold blue (or green, depending on your stain); whereas areas of edema will be a wispy light blue or maybe even light gray.
Finally, the last reason for spacing of tubules in the cortex is an interstitial infiltrate. The most common cause of an interstitial infiltrate is inflammation; however rarely you can have malignant interstitial infiltrates like lymphomas etc. In cases of heavy inflammation looking for the atrophic tubules on your special stains is helpful in distinguishing between acute interstitial nephritis (inflammation in non-fibrotic areas) versus chronic tubulointerstitial nephritis (inflammation in fibrotic areas). In many cases both can coexist.
Medullary rays
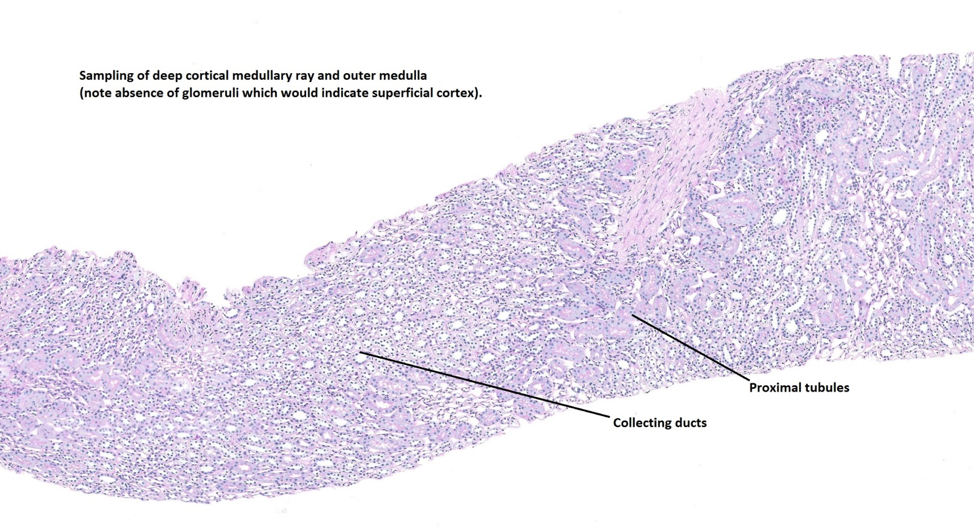
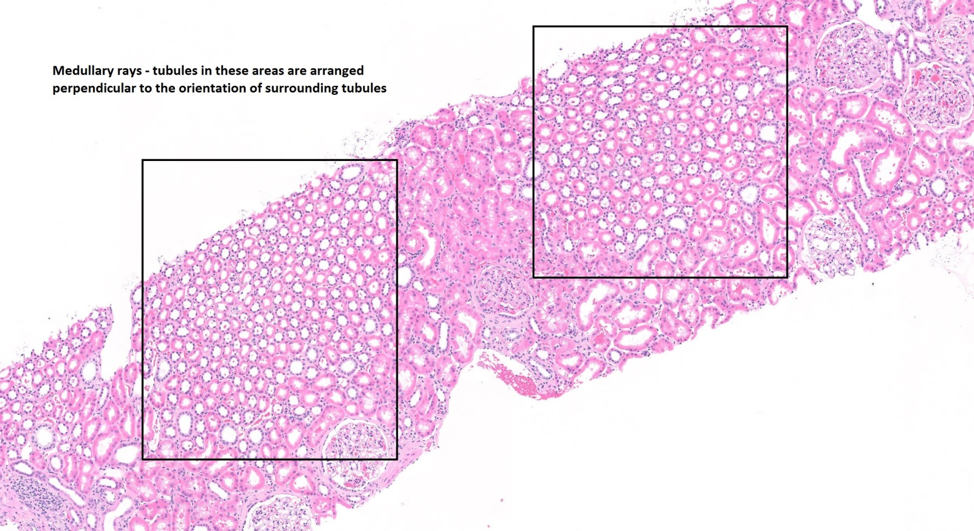
The medullary rays are extensions of the outer medulla which project into the cortex. In these areas the collecting ducts and straight portions of proximal and distal tubules are oriented at 90° angles (perpendicular) to the tubules in the cortical medullary junction. Sometimes biopsies taken by an accidental perpendicular approach to the renal capsule may predominantly sample medullary rays.
One pitfall to avoid here is interpreting the medullary rays as areas of tubular atrophy. This is because the medullary rays will contain collecting ducts which are normally slightly spaced apart with intervening amounts of rather prominent collagen (as described below).
Next month we will focus on the Medulla as Part 2 of What is Normal: The Tubulointerstitium
Post by: Vighnesh Walavalkar, MD (@vighnesh_w)
Renal Pathologist, UCSF Medical Center, San Francisco, CA
NSMC Intern 2019


An excellent article for both the beginner and the expert Nephrologist.