Introduction
Physical examination is a quick and inexpensive way of diagnosing stenosis and other causes of vascular access dysfunction. Its ability to reliably detect stenotic lesions compared with ultrasound and angiography (the gold standard), has repeatedly been demonstrated. Inspection, palpation, and auscultation are the three main elements of an arteriovenous (AV) access physical examination, which can be performed by nurses and physicians.
The Basics
An arteriovenous fistula (AVF) is made through the surgical connection of the patient’s native artery and vein. The site of this connection, the anastomosis, is the most distal portion of the fistula. After the fistula is created, the vein enlarges in response to increased blood flow from the feeding artery, forming a long, arterialized venous segment that is cannulated with needles for hemodialysis. Weak blood supply from the feeding artery may result in delayed or failed fistula maturation.
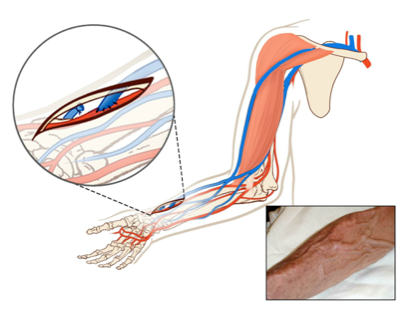
Figure 1. A radiocephalic fistula. From Atlas of Dialysis Vascular Access.
An arteriovenous graft (AVG) is a hollow, synthetic tube with one end surgically attached to the patient’s artery (arterial anastomosis) and the other attached to the vein (venous anastomosis). AVGs have either circular (loop) or linear (straight) configurations. The outline of an AVG is generally visible under the skin. When palpated, an AVG feels firm and ropey. Dialysis needles are placed in the graft rather than in the patient’s blood vessels. The venous anastomosis is the most frequent site for AVG stenosis, which has been attributed to multiple factors, including endothelial damage during surgical manipulation and high intra-access pressure from high blood flow.
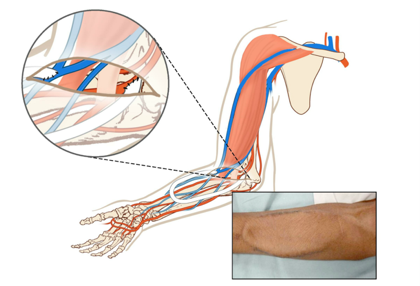
Figure 2 Loop graft in the forearm. From Atlas of Dialysis Vascular Access.
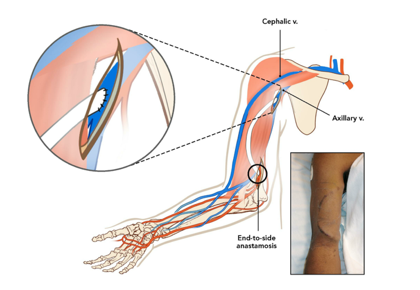
Figure 3 Straight graft in the upper arm. From Atlas of Dialysis Vascular Access.
Useful Terminology
Inflow refers to the feeding artery, the arterial anastomosis, and the juxta-anastomotic segment (the structures within 2 cm of the arterial anastomosis), whereas the outflow segment refers to either the entire draining vein until the subclavian vein in the upper extremity (Figure 4) or the native vein proximal to the venous anastomosis until the iliac vein in the lower extremity. Central veins include the subclavian vein, innominate vein, and superior vena cava in the upper torso and the iliac veins and inferior vena cava in the lower torso.
Figure 4 Anatomy of a fistula. From Vachharajani, Seminars in Dialysis, 2012.
Next Friday, we will focus on specifics of the physical exam
Post by: Crystal Farrington, ASDIN Fellow
Acknowledgments: This post is part of a collaboration between the Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. Special thanks to Tushar Vachharajani, Aisha Shaikh, Edgar Lerma, and the Education Committee of ASDIN for their comments and suggestions for this post. For more information about the ASDIN mission or membership, click here.


Very helpful study points which would greatly improve outcomes on fistula care