The use of urine sediment analysis is important for the diagnosis of glomerular hematuria. Red blood cells (RBC) casts, beautifully illustrated by @jrseltzer in last month’s post, usually confirm glomerular hematuria – but this is a rather special finding. Much more commonly, the diagnosis relies on the presence of dysmorphic, or glomerular-type, RBCs in the urine. Their presence can help avoid unnecessary urological procedures, may alert the clinician to the presence of glomerular injury, and is instrumental in the care of patients with kidney diseases. The presence of glomerular hematuria is usually established by microscopic examination of the urinary sediment.
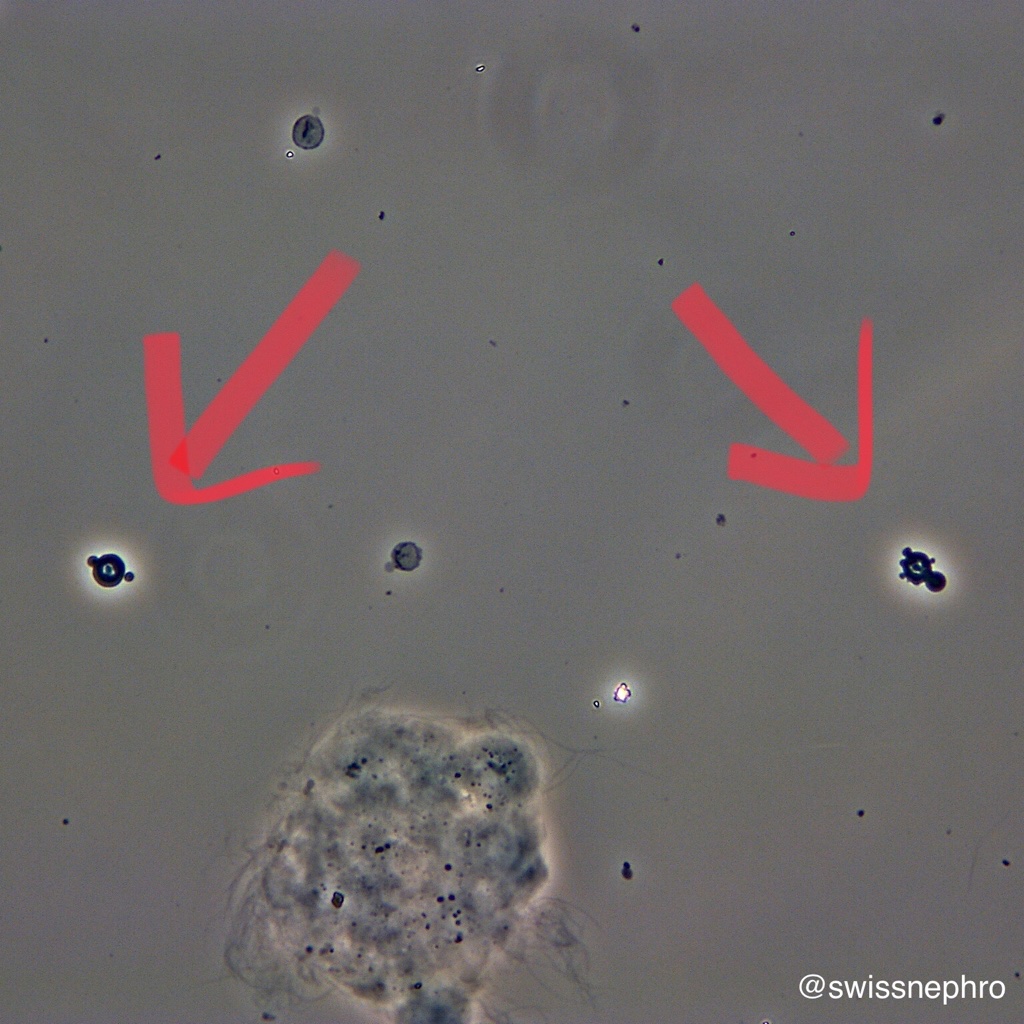
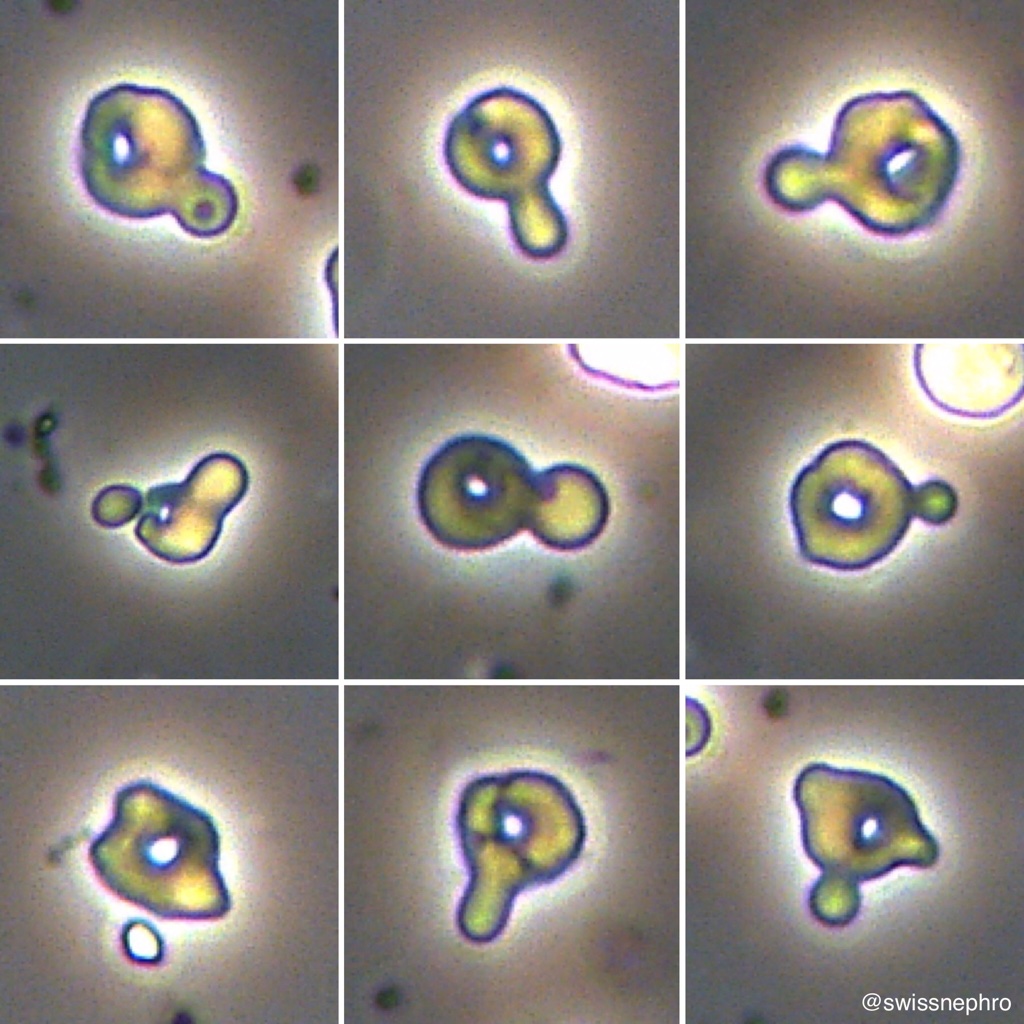
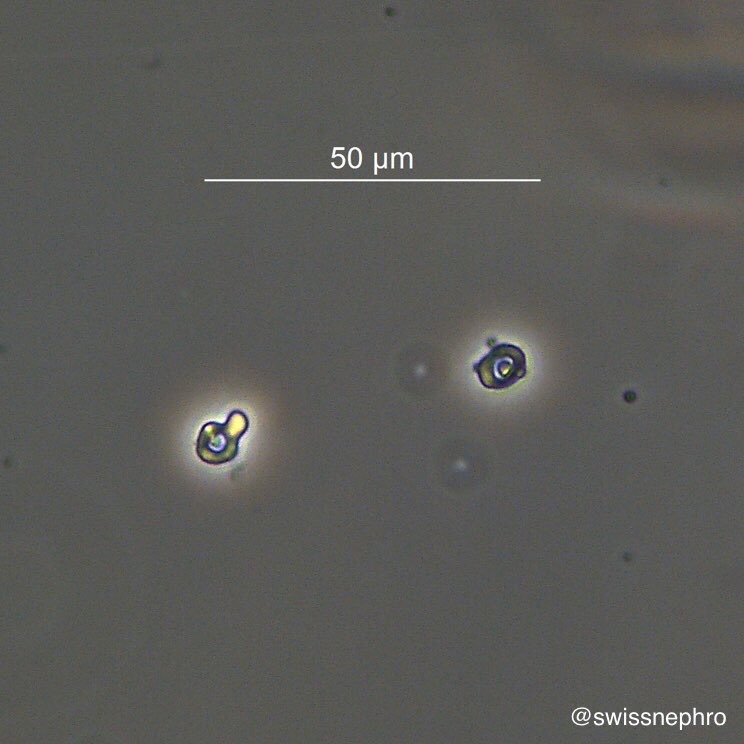
The term acanthocyte, one type of dysmorphic RBC, comes from the Greek word ἄκανθα (acantha) which means “thorn”. Thus, it refers to an RBC hat has a spiked cell membrane (see the figures 1-3 below). Acanthocytes represent the most distinguished shape of glomerular RBCs. They are best defined as ringforms (“doughnuts”) with external or internal protrusions. Acanthocytes are identified with good inter-observer agreement and show very high positive likelihood ratios for the presence of glomerular disease. A fraction of >=5% acanthocytes of all urinary RBCs is widely used to establish the diagnosis of glomerular hematuria.
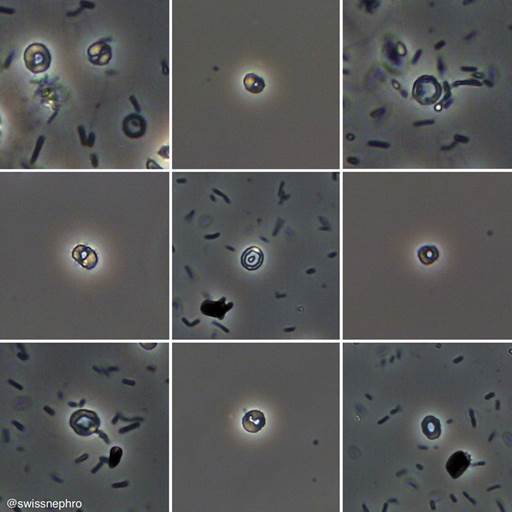
There is much less consensus about definitions and quantitative thresholds for other types of dysmorphic RBCs. My personal practice is as follows: In addition to acanthocytes, I count doughnut/ringform or target-like shaped RBCs without protrusions (Fig. 4) and – with restrictions – certain forms of destructed RBCs as dysmorphic. Usually, I only consider destructed erythrocytes when I have also seen some convincing ringforms or acanthocytes. With more than 30% ringforms I call it “definite” glomerular hematuria. When the 30% threshold is only reached by also counting destructed RBCs, I label it “possible” glomerular hematuria.
It is important to note that these percentages are only useful in patients with hematuria. Among the few RBCs excreted by healthy persons, the fraction of glomerular-type erythrocytes might be similarly high.
Post by: Florian Buchkremer, MD
Merci infiniment pour ces informations utiles
What type of stains and preparation for such type of samples?? And how do you report the result?? Am Heba Cytopathologist from Egypt
Really helpful for the diagnosis of GN 👍
You can use for instance 100 RBCs/hpf-many dysmorphic forms
it was really helpful. Asante sana
from Tanzania.
Thanks for this nice lecture , I hope to send me how u write the report of dysmrphic RBCs so u can inform the doctor by your result in a proper way . again thanks for this ,
from Egypt
Samer Abbas , MD