“You’ll come to learn a great deal if you study the insignificant in depth” ― Odysseus Elytis
In kidney transplant recipients, serum creatinine (SCr) remains the mainstay of allograft function assessment. Biopsy is the gold standard to diagnose dysfunction, but is an invasive procedure, not without risks and variability of diagnosis among pathologists reading a biopsy. Histological diagnosis can be discordant with established guidelines in as much as 30% cases, especially for antibody mediated rejection (ABMR). Presence of donor specific antibody (DSA) is a diagnostic criteria for ABMR but by itself, does not correlate with active injury. We have long awaited a non-invasive biomarker to detect allograft injury that precedes the rise in serum creatinine and can be used to diagnose rejection, adjust immunosuppression as well as monitor allograft function. Herein lies the excitement around donor-derived cell free DNA (dd-cfDNA).
Cell-free DNA is fragmented DNA in the plasma that originates from cells undergoing injury and death. It is extremely low in concentration, only a few thousand genomic copies/mL. Fetal DNA is known to be present in plasma of mothers and has been used in prenatal testing to screen for trisomies. Analogously, organ donor DNA can be found in recipient’s plasma in solid organ transplant recipients as well as urine of kidney transplant recipients. (Fig. 1).
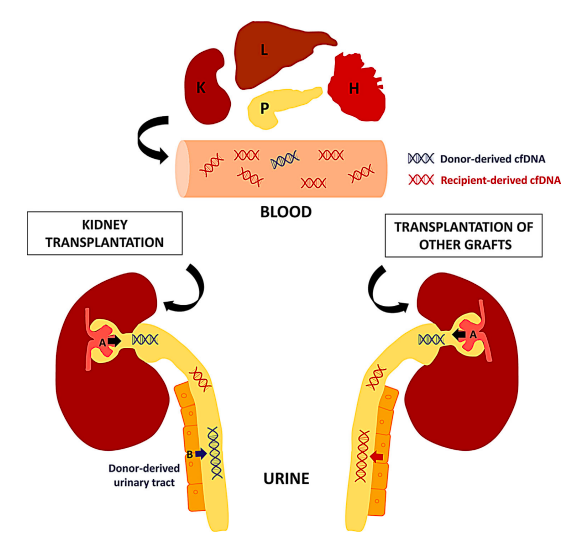
Figure 1. Origin of blood and urinary (donor-derived) cfDNA after solid organ transplantation.
Although it was first reported in the 1990s, accurate and validated analytical assays did not exist. Recent advances in PCR and next generation sequencing have made its detection feasible and cost effective. These techniques allow targeted amplification and sequencing of single-nucleotide polymorphisms (SNP) to quantify donor and recipient DNA contributions, in the absence of donor and recipient genotyping. The level of plasma dd-cfDNA in stable kidney transplant patients is usually less than 1%, with one study showing median of 0.21% (IQR 0.12%-0.39%). A serial change in the level more than 61% from the first value was considered outside the expected biological variation. The level increases after kidney transplant and decrease to about <1% by 2 weeks post-transplant. Levels are higher in deceased donor vs living donor recipients indicating reperfusion injury (Fig. 2). A subsequent increase can indicate organ injury. It decreases in response to treatment of rejection. Its role in allograft rejection is being actively studied in other solid organ transplants such as heart, lung and liver.
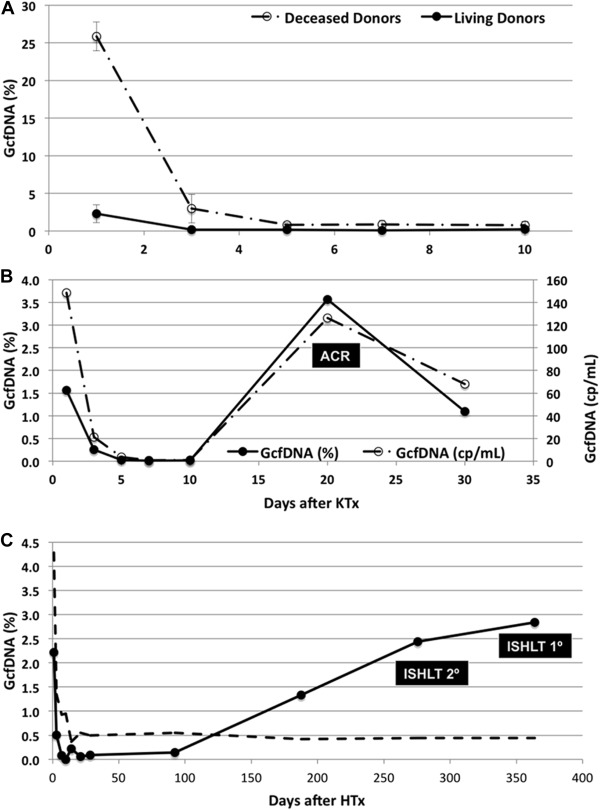
Figure 2. Graft derived cell free DNA (GcfDNA) level after kidney transplant (KTx).
DART study, by Bloom et al, was the first to report the utility of dd-cfDNA in kidney transplant recipients. In 102 patients with 107 for-cause biopsies having matched plasma dd-cfDNA, there were 27 rejection episodes. Median dd-cfDNA was 2.9% (ABMR), 1.2% (T cell–mediated Rejection TCMR >IB), 0.2% (TCMR IA), and 0.3% in controls (without histological rejection). At a cutoff point of >1%, it was able to discriminate rejection from no rejection as well as ABMR from non-ABMR rejection (Table 1). One important point to note is that this assay was elevated in TCMR>1B but not TCMR 1A. The study concluded that dd-cfDNA may be used to assess allograft injury and level <1% reflected absence of active rejection (TCMR >IB or ABMR).
In another analysis from the DART study of dd-cfDNA with paired DSA samples in clinically indicated biopsies, Jordan et al showed that at in DSA positive patients, dd-cfDNA performed better for diagnosis of ABMR(Table 1). It concluded that patients with dd-cfDNA+/DSA+ results have high probability of active ABMR (Fig. 3)
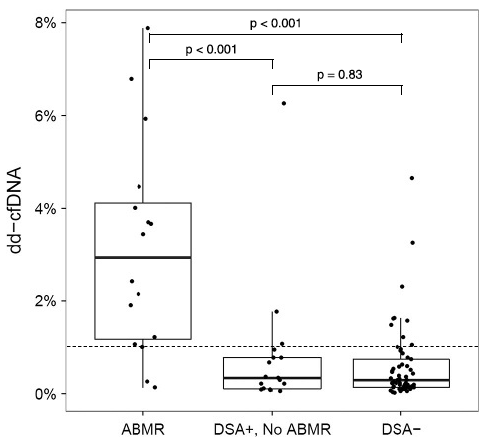
Figure 3. dd-cfDNA level is significantly higher in patients with DSA+ Active ABMR patients.
Sigdel et al in their retrospective study used a different, SNP-based massively multiplexed PCR assay and were able to discriminate active rejection (both ABMR and TCMR) from non-rejection status (Table 1). The results were similar for protocol biopsies vs for-cause biopsy samples, living vs deceased donors and importantly, showed the ability to distinguish both ABMR and TCMR cases (>1A) from borderline rejection or other injury including toxic injury or viral infection
In the abovementioned studies, dd-cfDNA performed better than Scr or eGFR alone in diagnosing rejection.
| Table 1. Diagnostic performance of dd-cfDNA in different studies | ||||||
| Study | Rejection Type | AUC-ROC | Sensitivity | Specificity | PPV | NPV |
| Bloom et al | Active RejectionABMR or TCMR>1B | 0.74 (0.61 – 0.86) | 59 (44 – 74) | 85 (79-91) | 61 | 84 |
| ABMR vs Non-ABMR | 0.87 (0.75 – 0.97) | 81 (67 – 100) | 83 (78-89) | 44 | 96 | |
| Jordan et al | ABMR or mixed | 0.86 (0.7 – 0.98) | 81 (67-100) | 82 (67-100) | 81 | 83 |
| Sigdel et al | Active RejectionABMR or TCMR>1A | 0.87 (0.8 – 0.95) | 89 (78 – 100) | 73 (65 – 80) | 52 | 95 |
Like every diagnostic test, the result has to be interpreted with the right context and its limitations understood. Since dd-cfDNA increases with allograft injury, the effects of BK nephropathy, glomerulonephritis or active urinary tract infection on its level need further evaluation. At this time, its use in patients with multiple-organ transplants is not recommended although a recent study of 12 repeat kidney transplant recipients with retained allografts showed that ‘combined’ dd-cfDNA is <1% with no rejection and higher in patients with biopsy proven rejection. In addition, it should not be checked in recipients of a transplant from a monozygotic twin or allogenic bone marrow transplant. Level drawn right after a kidney biopsy can be falsely elevated and should be interpreted with caution. Lastly, its ability to accurately predict TCMR should be further evaluated.
Advantage of dd-cfDNA lies in its high NPV, which in the absence of DSA, reduces the need for a biopsy and prevents ambiguity in diagnosis. In addition, when used in conjunction with DSA, it increases the pre-biopsy probability of ABMR aiding decision-making process. Rise in its level precedes SCr changes and allows for early detection and its use as a screening tool. Lastly, it also allows for convenient and non-invasive longitudinal monitoring of response to intervention, as compared to repeated biopsies.
We could see increasing use of dd-cfDNA in coming years. Future studies should include large cohort of cases with different diagnoses as well as assess effect on clinical outcomes of treatment strategies based on utilizing dd-cfDNA versus traditional methods. The ongoing study titled ‘Evaluation of Patient Outcomes from the Kidney Allograft Outcomes AlloSure Registry (KOAR)’ would definitely serve this purpose.
I would like to thank Principal Pod mentor @NatashaNDave for her generous help with the write-up and Dr. Daniel Brennan for being an eternally inspiring mentor and teacher. @NSMC Internship Rocks.
Anshul Bhalla (@BhallaAshul)
Transplant Fellow
Johns Hopkins Hospital
NSMC Intern 2019