Last month, we focussed on the renal cortex in the tubulointersitium, as part of the Kidney Biopsy of the Month: What is Normal series.
We will now concentrate on the renal medulla, a region of the kidney sometimes overlooked in renal pathology reports. There are certain pathologic changes that can be seen in the medulla, and therefore knowing the normal architecture is important.
A quick recap of the basics first:
The tubulointerstitium of the kidney is broadly divided into the renal cortex and the renal medulla. These are extremely important components of the kidney, which can show a broad spectrum of changes ranging from subtle to significant, in both acute and chronic kidney injury. Therefore in order to recognize the pathologic changes in these areas, one must first be familiar with its normal architecture.
In this post, we will cover the main histologic features of the normal tubulointerstitium as seen on diagnostic renal biopsies. For a more in-depth review please refer to my favorite references for renal pathology: Heptinstall’s Pathology of the Kidney, Silva’s Diagnostic Renal Pathology and Renal Pathophysiology, The Essentials.

1 = Renal corpuscle including Bowman’s capsule and the glomerulus
2 = Proximal convoluted tubule
3 = Proximal straight tubule
4 = Descending thin limb
5 = Ascending thin limb
6 =Distal straight tubule (thick ascending limb)
7 = Macula densa located within the final portion of the thick ascending limb
8 = Distal convoluted tubule
9 = Connecting tubule. Connecting tubule of the juxtamedullary nephron that forms an arcade
10 = Cortical collecting duct
11 =Outer medullary collecting duct
12 = Inner medullary collecting duct
Renal Medulla
Architecturally, the renal medulla is divided into an outer segment and an inner segment. The outer medulla is further divided into an outer stripe and an inner stripe.
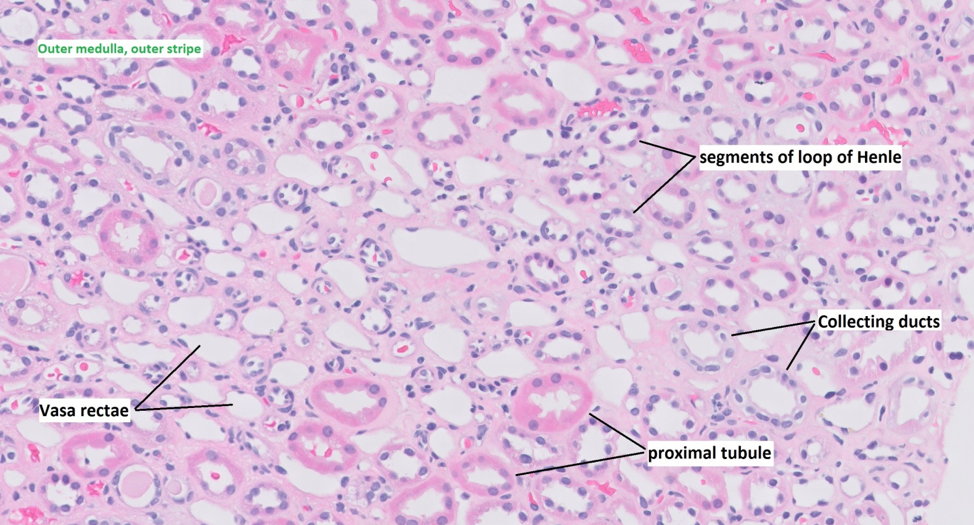
Outer medulla
Outer stripe: The outer stripe contains straight portions of the proximal tubule, collecting ducts and the thick ascending loops of Henle. The outer stripe of the outer medulla has structures similar to the medullary rays of the cortex.
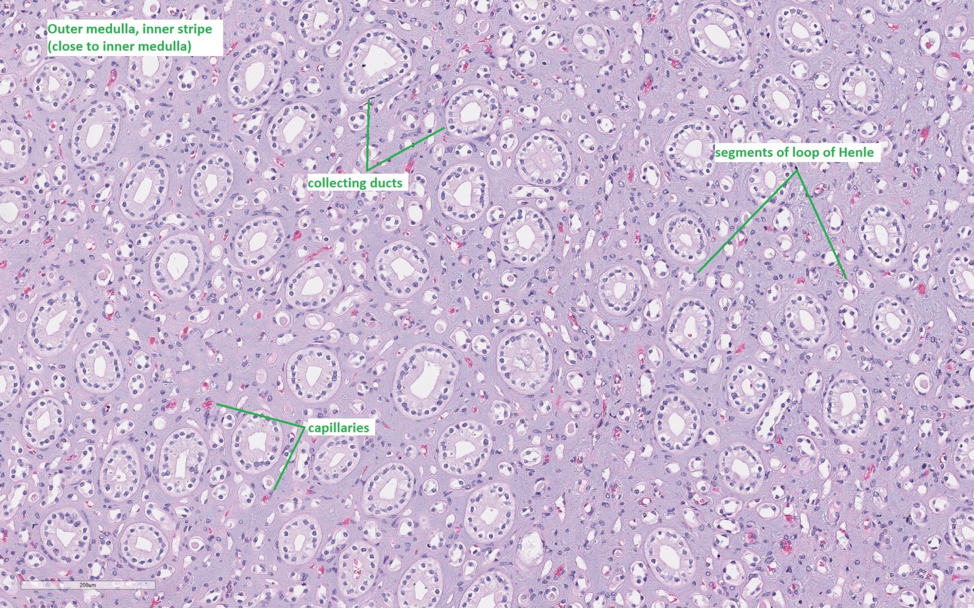
Inner stripe: The inner stripe contains the thin descending and thick ascending loops of Henle as well as collecting ducts.
Inner medulla
The inner medulla has the thin descending and ascending loops of Henle, as well as the large collecting ducts of Bellini.
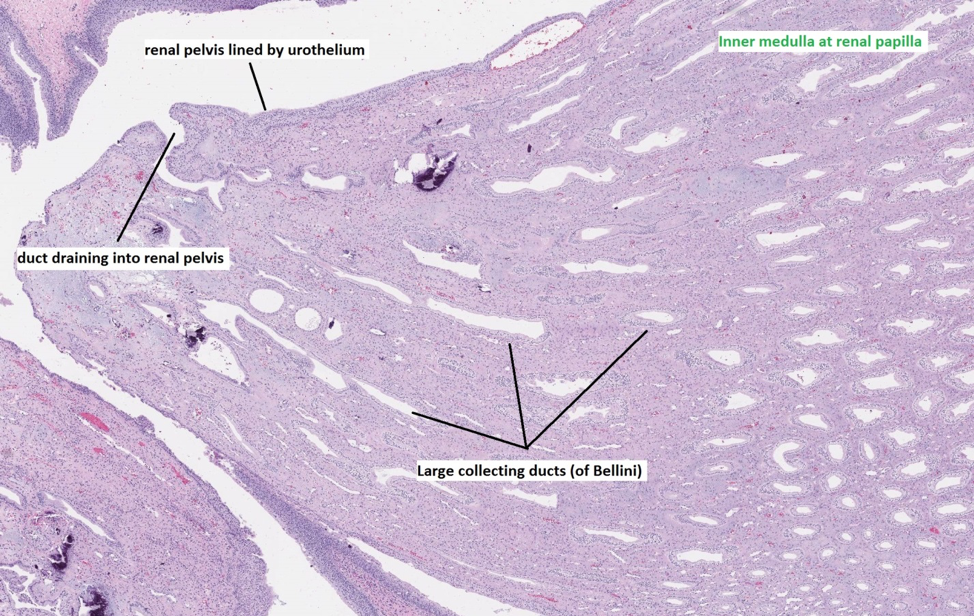
The interstitial area in the medulla appears slightly more prominent, i.e.: the medullary structures such as collecting ducts are more widely (but regularly) spaced due to the presence of abundant interstitial collagen. This amount of collagen is normal and should not be interpreted as “interstitial fibrosis” or chronicity.
Renal amyloidosis can often affect the medulla and in some cases are medullary predominant (eg: Apolipoprotein A-I). Therefore any irregular spacing of medullary structures or abnormal staining with trichrome should prompt consideration for a Congo red stain.
Interspersed within the collecting ducts and segments of the loop of Henle are small capillaries called the vasa rectae. There are no arteries, veins or lymphatics in the renal medulla. The vasa recta are usually empty without inflammatory cells. Passive inflammatory cells within vasa rectae can be commonly seen in acute tubular epithelial cell injury (ATN) of the renal cortex. Therefore if you start to notice prominent inflammatory cells within the medullary capillaries go back to the renal cortex and look for features of acute tubular epithelial cell injury.
Another pitfall to avoid is calling inflammation in medullary capillaries as “peritubular capillaritis” in transplant kidney biopsies showing ATN (e.g: delayed graft function). An extremely important histologic lesion in the medulla is that of renal medullary angiitis, which may be confused for nonspecific inflammation or AIN.
Renal medullary angiitis is a rare lesion often associated with systemic vasculitides like ANCA vasculitis. It is characterized by interstitial hemorrhage in the medulla, medullary inflammation, and most specifically, karyorrhectic debris around medullary capillaries. Identifying this lesion in suboptimal biopsies (those without many glomeruli), is very helpful in diagnosing ANCA associated vasculitis in the correct clinical setting.
The renal medulla is also an important location for identifying tubular casts such as granular casts and red blood cell casts; as well as atypical casts such as light chain casts, bile pigment casts, myoglobin casts etc. Finally occasional neutrophilic microabscesses may be seen within medullary collecting ducts which may indicate a component of ascending acute pyelonephritis; and when severe may even be present cortical tubules as well.
Vighnesh Walavalkar, MD
Renal Pathologist, UCSF Medical Center, San Francisco, CA
NSMC Intern 2019


i think that fig1 is inner strip; fig 2 is inner medullary, fig 3 is papilla