We recently took over the care of a 20 year old man of Asian origin who was admitted under the surgical team. He presented with 4 days of bilateral, colicky loin pain. He had no past medical history or family history and took no regular prescribed medications. He had just returned from a 2 week holiday where he had consumed an excessive amount of alcohol. He did not use any recreational drugs, but had taken ibuprofen for his pain over the preceding 3 days. His urine dipstick on admission showed no blood or protein. His serum creatinine was elevated at 171 umol/l (1.93 mg/dL) and did not improve with intravenous fluid. Serum urate was minimally elevated at 0.45 mmol/l (7.6 mg/dL) and creatine kinase was normal. A kidney ultrasound scan showed normal sized kidneys without obstruction.
He underwent a computed tomography (CT) scan with contrast on the day of admission which showed abnormal enhancement of the kidney parenchyma in arterial and portal venous phases, raising the possibility of microvascular impairment (Fig. 1). Repeat imaging by non-contrast CT 24 hours later demonstrated areas of residual contrast enhancement corresponding to hypoperfused areas in both kidneys on the previous scan. The radiology report described the “features as those that can be seen in ALPE.”
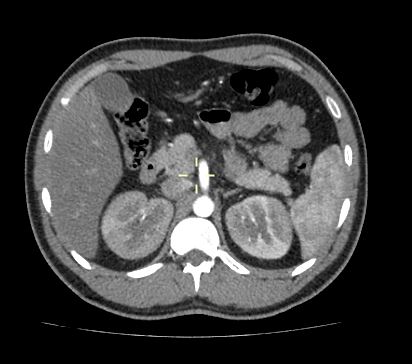
But what is ALPE? It sadly isn’t part of a French ski resort, standing for “acute kidney injury with loin pain after anaerobic exercise.” It was first described in 2002 and is caused by severe vasoconstriction in the kidney with resultant ischemia. Diagnosis is comprised of both clinical and radiological features. Acute kidney injury occurs with minimally elevated creatine kinase and myoglobin levels, with loin pain typically occurring several hours after intense anaerobic exercise. Persistent wedge-shaped areas in the kidneys are seen on plain CT up to 72 hours following the administration of contrast media.
The main described risk factor is “renal hypouricemia”, due to defective uric acid reabsorption or secretion – it can be inherited in an autosomal recessive pattern, with a greater prevalence in Asian populations. However, the precise mechanism involved remains elusive. Uric acid levels can be normal or mildly elevated at the time of AKI.
ALPE doesn’t always have to occur after anaerobic exercise, however – it has also been described as occurring after excess alcohol (as in this case), analgesic use, and upper respiratory tract infections. Interestingly, our patient described similar loin pains when in the gym doing repetitive weight lifting. The pain lasts on average 3-4 days, which roughly correlates to the time when peak serum creatinine is seen. In our patient, serum creatinine peaked at 220 umol/l on the 5th day from onset of pain. He was allowed home with early review, and by day 10 creatinine had fallen to 90 umol/l.
The prognosis is good – although some individuals do require short-term renal replacement therapy. Approximately 20% of patients develop recurrent episodes if exposed to similar triggers, but there are reports of individuals going on to have successful careers as professional athletes in sports such as cycling after a diagnosis of ALPE.
We’ve seen several young patients develop painful AKI after a period of alcohol excess – and a smaller number of cases occurring after intense exercise – and I suspect this mechanism is causative in at least some of the “Saturday night out” AKIs we see.
(Case presented with patient consent)
Post by: Ailish Nimmo, Nephrology SpR, Edinburgh

Thank you
ALPE- acute kidney injury with loin pain after anaerobic exercise
What is the Abbreviation ALPE?
Thank you