Clinical Scenario 1:
Mr.T is a 68 year old male with long standing uncontrolled Type 2 diabetes mellitus complicated by diabetic retinopathy and neuropathy. Over the years he has had progression of chronic kidney disease with subnephrotic range proteinuria. His creatinine last year was fluctuating around 2.8 mg/dl. You are evaluating him in the office. His blood work from 1 month ago showed a creatinine of 3.9 mg/dl. He was taken off lisinopril, told to hold lasix and to drink more water. One week ago he had repeat blood work done showing creatinine up to 5.6 mg/dl with eGFR of 9 ml/min. He is accompanied by his wife who reports he has been having slurred speech for the last few days and ‘just does not seem like himself’. The patient denies acute symptoms but does report decreased appetite and lack of sleep. The rest of his biochemical profile is significant for potassium of 5.7, BUN 89 and bicarbonate of 17. On physical examination he has a friction rub in the precordium. You counsel the patient about his imminent need to start dialysis. He has had dialysis education done and is in agreement to proceed with hemodialysis initiation.
1. What dialysis vascular access option is available for this patient other than a tunneled dialysis catheter (TDC)?
Mr.T is developing signs of uremia and needs to start hemodialysis urgently Due to the urgent need for hemodialysis, the patient will need a vascular access that is ready for immediate use. An Arteriovenous Fistula (AVF) can take up to 6-12 weeks for maturation. Mr. T undergoes vessel mapping, and he does not have adequate veins for creation of an AVF in his upper extremities. Based on the vessel mapping findings, the best AV access for him would be an upper extremity Arteriovenous graft (AVG). A conventional ePTFE AVG can typically be cannulated 2-3 weeks after placement. But given that Mr. T has developed uremic symptoms, he needs to start dialysis immediately. Up until a few years ago, the only vascular access that could be used immediately after placement was a tunneled dialysis catheter (TDC). However, now there is another option available, the ‘Early Cannulation Arteriovenous Graft” (ECG). ECG’s can be cannulated safely within 72 hours after implantation This approach results in complete avoidance of TDCs, which are known to be associated with higher morbidity due to the associated risk of bacteremia and even death Early Cannulation AVGs not only allow for complete avoidance of TDCs but in some cases allow for early removal of the TDC
A prospective multi-center study published in August 2015 showed that early cannulation AVGs can be safely cannulated soon after implantation (usually within 3 days), without significant difference in patency and complication rates compared to the conventional ePTFE grafts as described in the published literature.
2.What is the primary and secondary patency rate for Early Cannulations Grafts?
Julien Al Shakarchi published a systematic review and meta-analysis that looked at 19 studies involving different ECGs including Flixene, Avflo, Acuseal and Vectra grafts. Primary patency rates ranged from 40-60% and secondary patency ranged from 70-85%. This systematic review suggests that the patency of the early cannulation graft is comparable to the conventional ePTFE AVG, though long term data is lacking T Patency rate comparison for the different types of ECGs is not available as there have been no head-to-head trials..
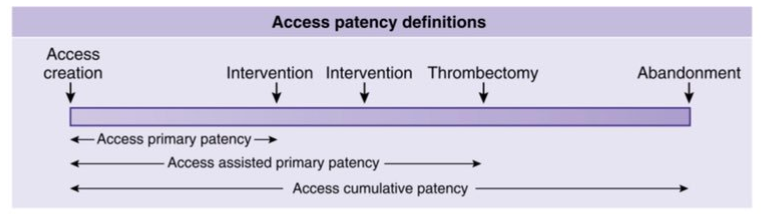
Of note, primary patency (intervention-free access survival) refers to interval from time of access placement to any intervention designed to maintain or reestablish patency or to access thrombosis. Secondary patency or access cumulative patency refers to interval from time of access placement to access abandonment, including intervening manipulations (surgical or endovascular interventions) designed to reestablish the functionality of thrombosed access)
Reference: https://www.ncbi.nlm.nih.gov/pubmed/29487092
3.What is the economic impact of the early cannulation grafts (ECGs) and how do they compare to AVFs and TDCs ?
As per this study published by Desai et al in January 2019, the average cost of care was $17,523 for AVF compared to $5,894 for early cannulation graft. This cost difference was due to fewer TDC related complications in patients with ECGs, and also due to fewer n early interventions needed in ECGs compared to AVFs. Less use of TDC led to cost-savings of about $2 million per year for ESRD patients. This was due to decrease in expenditure associated with sepsis, decreased length of hospital stay and decrease in ICU utilization, In addition, the same author reported a 1-year survival advantage for ECGs compared to AVFs The ECGs are more expensive than conventional AVGs, but unlike the conventional AVGs, the ECGs can be used for dialysis immediately after placement, this in turn results in complete avoidance of TDCs. The avoidance of TDC results in cost-savings, for reasons mentioned above, thereby justifying the higher cost of ECGs over a conventional AVGs
Clinical Scenario 2
Mrs.CVS is a 67 year old female with end stage kidney disease for the past 17 years secondary to hypertensive nephrosclerosis and diabetic nephropathy. Her other comorbidities include type 2 DM, congestive heart failure with preserved ejection fraction and multiple admissions for sepsis related to diabetic foot ulcers and osteomyelitis of the metatarsal bones. She has been subjected to multiple central venous catheters during her hospitalizations including PICC lines for long term antibiotic treatment. 18 years ago she had a left forearm radiocephalic arteriovenous fistula created but it failed to mature despite balloon assisted maturation procedure. She then had a left upper arm arteriovenous graft placed through which she has been getting intermittent dialysis. Lately the graft has thrombosed recurrently and was found to have significant calcification. She also has multiple pseudo-aneurysms and scar tissue at the cannulation site. The nephrology and vascular team intend on creating new access but prior vein mapping has shown >90% stenosis of the right subclavian vein, therefore that side was avoided for AVF/AVG creation. Mrs. CVS has been referred to transplant and is on the waiting list. She has a history of ventral hernias, one of which was incarcerated, therefore she is not deemed a good peritoneal dialysis candidate.
1.Which dialysis vascular access would be most appropriate for this patient?
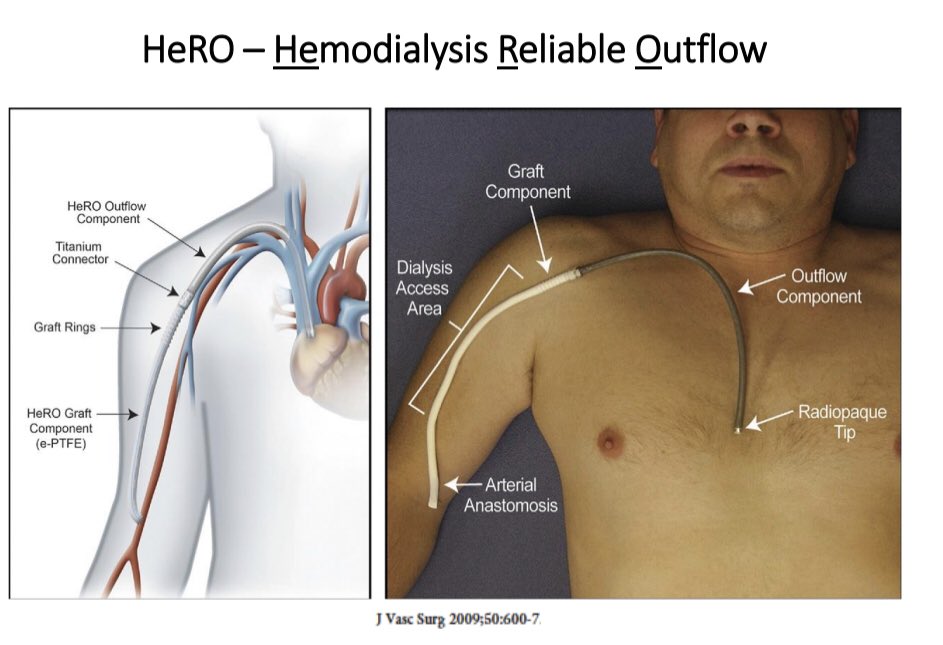
Tunneled dialysis catheters have high infection rates, and with the patient’s history of recurrent sepsis, one should avoid placing a TDC as that will increase her chances of bacteremia and systemic infections. A HeRO graft (Hemodialysis Reliable Outflow) is a good choice for an AV access in the setting of central vein stenosis. The HeRO graft comprises a ‘graft’ component (which is subcutaneous and can be used for hemodialysis access), a ‘connector’ and a ‘catheter’ component which bypasses the central stenosis and serves as an outflow channel. Unlike the TDC, the HeRO graft is fully subcutaneous AVG. One can only cannulate the ‘graft component’ of a HeRO graft and not the ‘catheter component’. For successful HeRO graft placement, the surgeon has to be able to traverse the central vein stenosis with the catheter-portion of the HeRO graft
2. Is there any cost benefit of using the HeRO graft instead of a TDC?
Yes. Although the initial cost of placing a HeRO graft is more than TDC placement, the HeRO graft has better long term patency and lower complication rate than a TDC which results in cost-savings in the long run In a study that performed a cost analysis of HeRO grafts, a cohort of 100 patients, patients with a HeRO graft had 6 fewer access-related complications, 53 fewer access-related infections and 67 fewer device thrombosis as compared to patients with TDC’s.
3.Why place an upper extremity HeRO graft instead of a lower extremity femoral AVF or femoral AVG?
Studies that have compared upper extremity HeRO grafts to lower extremity femoral AVFs and AVGs have been retrospective in nature Therefore, the quality of evidence to make a definite comparison between the HeRO grafts and femoral AVFs/AVGs is weak. Given the available evidence, which shows comparable patency between HeRO graft and femoral AVG, along with the convenience of an upper extremity AV access, most clinicians and patients prefer an upper extremity HeRO graft over a lower extremity femoral AVG. Some centers may prefer to place a femoral AVF instead of an upper extremity HeRO AVG, but femoral AVF placement requires surgical expertise which some centers may not have. In addition, the patients need to be monitored closely for lower extremity steal syndrome after femoral AVF creation
For further details on the topic of ‘HeRO grafts’ please refer to comprehensive tweetorial by @Aishaikh on HeRo grafts.
Bhavnish Bucktowarsing, MD
ASDIN Fellow
Acknowledgments: This post is part of a collaboration between the Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. Special thanks to Tushar Vachharajani, Aisha Shaikh, Edgar Lerma, and the Education Committee of ASDIN for their comments and suggestions for this post. For more information about the ASDIN mission or membership, click here. We would also like to thank Anil Agarwal, Robin Shah, Nabil Haddad, Khaled Boobes for assisting with this post.
Please note: these cases are vignettes created for educational purposes and patient consent has been obtained by author for clinical images.

Where should the dialysis technician insert the needles for dialysis? Am I correct in assuming that the needles pierce the skin on route to the graft portion of the apparatus?
How much pain is involved, compared to needle use with a conventional graft?
Very informative.
Awesome