Welcome to our inaugural post- every month we will posting a synopsis based on a Glom Con conference.
In this GlomCon Conference, Dr. Stephen M. Korbet reviewed the “Prognosis and Management of Primary FSGS”. Our Moderator’s Notes are derived from his live presentation which you can view here.
Background
Focal Segmental Glomerulosclerosis (FSGS) has become the leading cause of primary nephrotic syndrome in the United States with increasing incidence worldwide. African-americans remain at the highest risk for FSGS as compared to other patient populations. Primary FSGS is now considered the most common cause of glomerulonephritis-related ESRD in the US.
Etiology and Clinical Classification
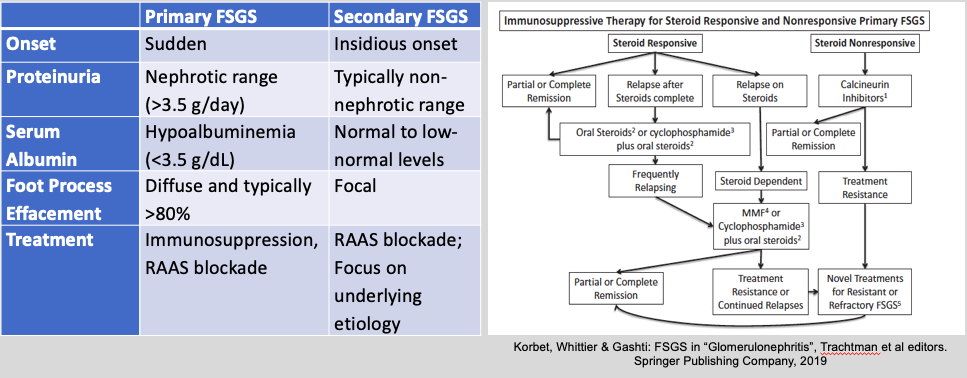
The lesions of FSGS are routinely subdivided into either primary (or often termed “idiopathic”) FSGS vs secondary FSGS forms.
- Primary FSGS is thought to be due to an unknown circulating factor. Patients with primary FSGS usually present with nephrotic range proteinuria (>3.5g/day), serum albumin less than 3.5 g/dL, and will have have diffuse foot process effacement (>80%) on electron microscopy (EM).
- Secondary FSGS is thought to be due to various different pathogenic mechanisms including via primary alterations of the glomerular epithelial cell, reduced nephron mass or glomerular adaptation, and secondary to focal proliferative glomerulonephritis. Patients with secondary FSGS typically present with non-nephrotic proteinuria, normal to low normal serum albumin >3.5 g/dL, and with segmental foot process effacement on EM. Common reported causes of secondary FSGS are:
- Viral: HIV-associated nephropathy, Parvovirus B19, BK virus, Epstein-Barr virus
- Drugs: Heroin-associated nephropathy, pamidronate, lithium, anabolic steroids
- Systemic: Lupus, IgA nephropathy
- Malignancy: Lymphoma, leukemia
- Genetics: Familial FSGS, sporadic genetic mutations, APOL1
- Reduced nephron mass / glomerular adaptation: Nephrectomy, reflux nephropathy, obesity-related glomerulopathy
Treatment Considerations
The general approach to patients with FSGS is treatment with renin-angiotensin-aldosterone (RAAS) blockade, good blood pressure control, and focus on any treatable secondary cause (if applicable). Patients with primary FSGS who have nephrotic syndrome are considered for treatment with immunosuppression.
Choice of Immunosuppression – a series of studies were reviewed, the regiments of which are highlighted here. This, however, does not represent any specific treatment recommendation by the speaker, the author, or GlomCon. There are guidelines (i.e. KDIGO) and review articles that also provide further guidance on therapeutic options.
- The standard therapy is prednisone 1 mg/kg/d (max 80 mg) or 2 mg/kg every other day for a minimum of 4 weeks and a maximum of 16 weeks or until complete remission, whichever is first. If there are contraindications to steroid use (examples include morbid obesity, uncontrolled diabetes, and/or prior steroid intolerance) then calcineurin inhibitors should be considered for the initial therapy (with or without low dose steroids).
- Relapsing FSGS: These patients can be treated with another course of high dose steroids or with cyclophosphamide with low dose steroids.
- Steroid dependent FSGS: These patients can be treated with (1) cyclophosphamide with low dose steroids, (2) rituximab, or (3) mycophenolate.
- Steroid-resistant FSGS is defined as the persistence of nephrotic syndrome after 16 weeks of prednisone at a dose of 1 mg/kg/day. These patients should be treated with cyclosporine 3-5 mg/kg/d in two divided doses for 4-6 months. If there is a partial or complete remission, then cyclosporine should be continued for 12 months followed by a slow taper. The relapse rate is high with discontinuation.
- Plasmapheresis works best in transplant patients with recurrent FSGS before the development of segmental scars.
Prognosis
Spontaneous remissions are rare in primary FSGS patients (<5%, and usually partial remission only). However, even partial remissions have shown to have better long term outcomes when compared to no remission at all. The following are important points to consider when determining the long term renal prognosis in primary FSGS patients:
- Non-nephrotic FSGS patients have a better prognosis compared to their nephrotic FSGS counterparts. Patients with massive proteinuria, >14 g/day, progress very rapidly to ESRD, sometimes termed as malignant FSGS.
- Higher serum creatinine >1.3 mg/dL, interstitial fibrosis >20% and presence of cellular lesions >1% are predictors of progression to ESRD.
- The APOL1 risk status has not been shown to influence response to initial treatment.
Author: Swati Arora, MD
Editor: Pravir V. Baxi, MD
Further Reading
1. Treatment of primary FSGS in adults. Korbet SM. J Am Soc Nephrol. 2012.
2. Focal Segmental Glomerulosclerosis. Rosenberg AZ, Kopp JB. Clin J Am Soc Nephrol. 2017.
Hi sir /mam
May i get case discussion on cryo gn ??