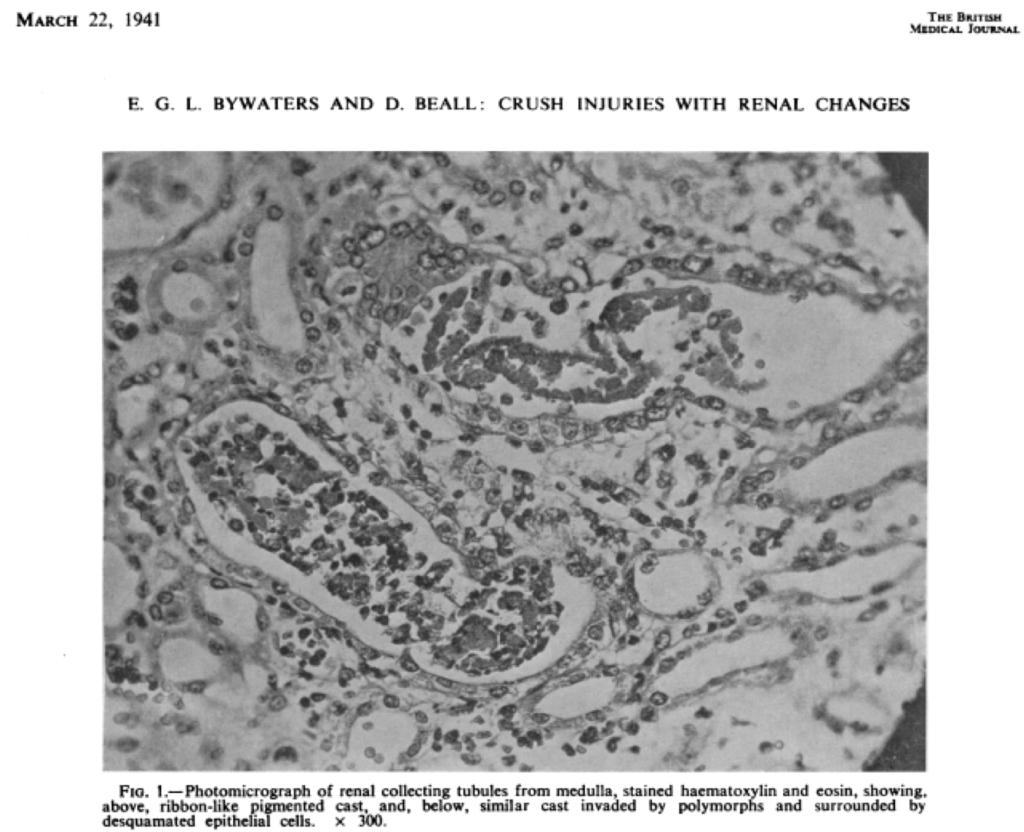
Eric Bywaters was the first to use the nomenclature “pigmented casts” in a 1941 British Medical Journal publication about crush syndrome where he illustrates pigmented casts (due to myoglobin) with a photomicrograph (Figure 1) of the kidney biopsy [1-3].
The literature on pigmented casts is sparse, thought there are at least 4 references [4-7] on this subject and all use the same kind of classification for pigmented casts:
- Myoglobin casts
- Hemoglobin casts
- Bilirubin/bile casts
Here, I will describe cast pigmentation due to endogenous pigments (myoglobin, hemoglobin, bilirubin/bile) and also a drug related pigment (phenazopyridine).
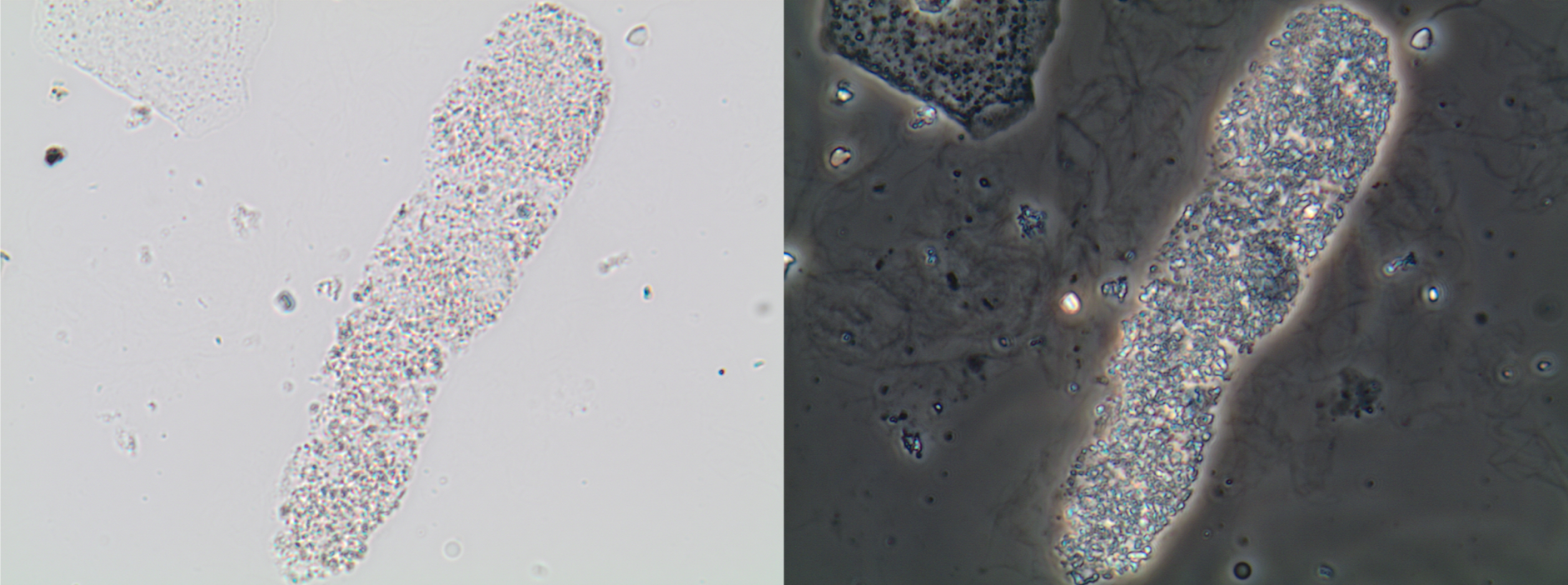
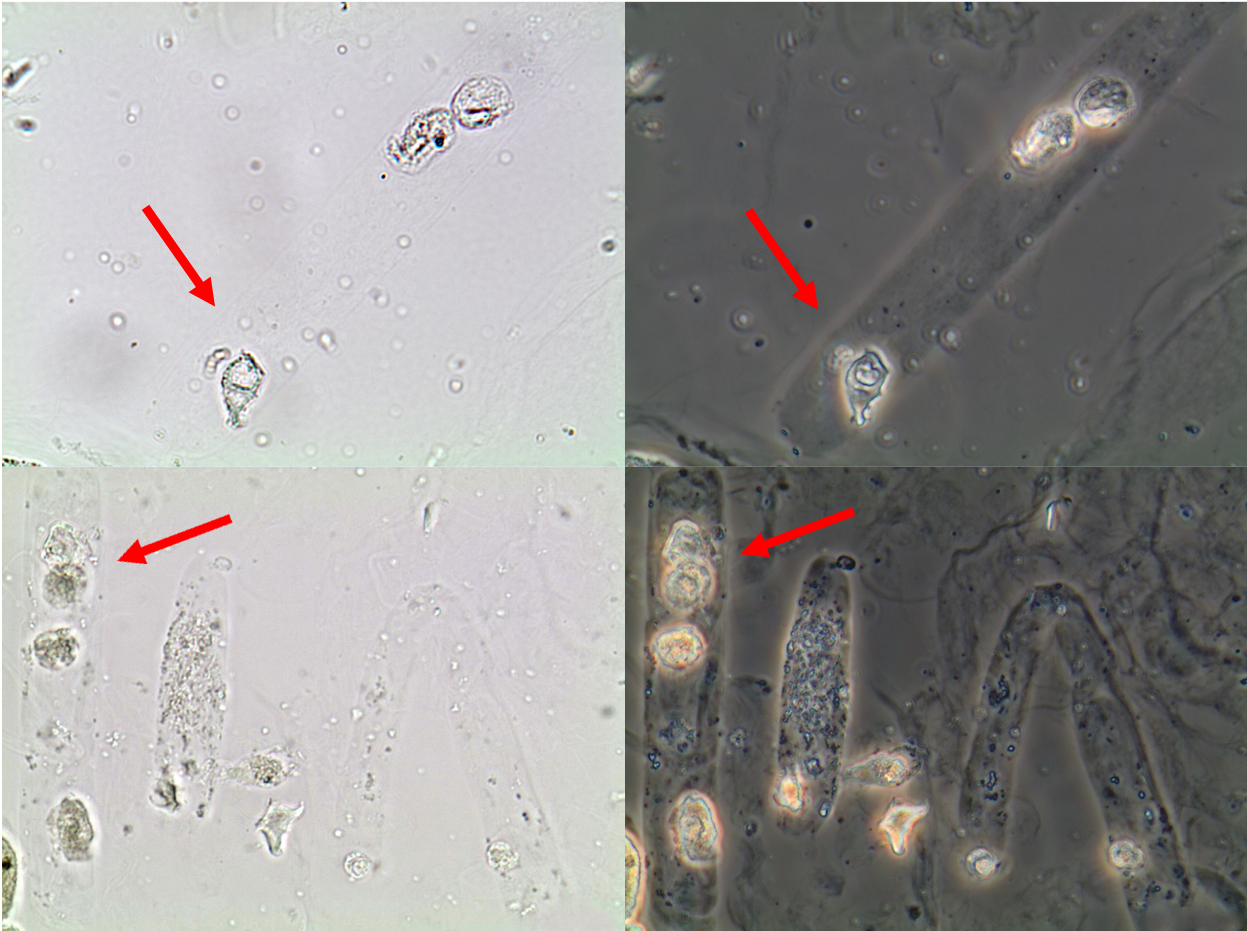
First, it is important to illustrate the color of urinary casts without pigments. Figure 2 illustrates the usual color of granular casts; Figure 3 illustrates the usual color of renal tubular epithelial cell (RTEC) casts; and, Figure 4 illustrates the usual color of waxy casts. As can be seen in the images, granular and RTEC casts present a greyish color scale and the waxy cast presents a yellowish/greenish/grayish color scale.

In general, the types of pigmented casts that are often observed in the urine sediment are RTEC, granular, and waxy casts.
Of note, muddy brown casts will not be covered here since they were covered previously in a Renal Fellow Network post.
Myoglobin Casts
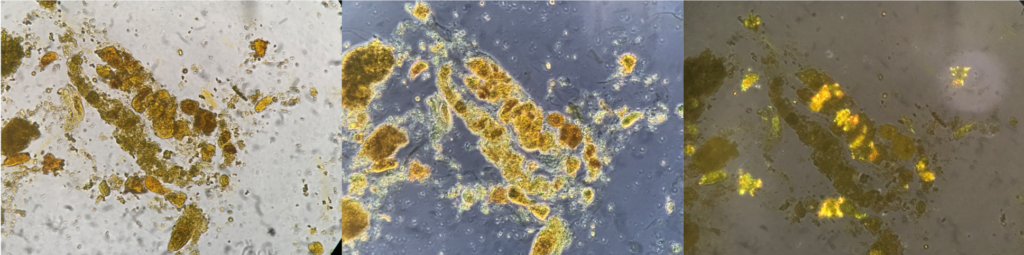
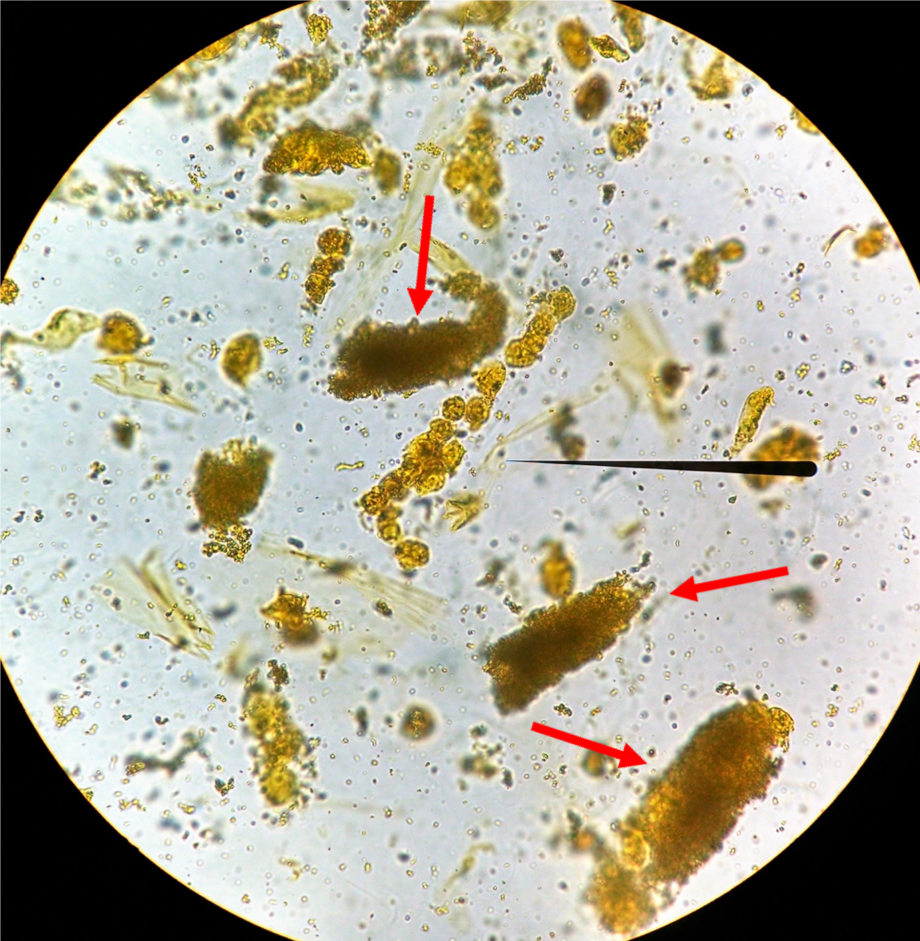
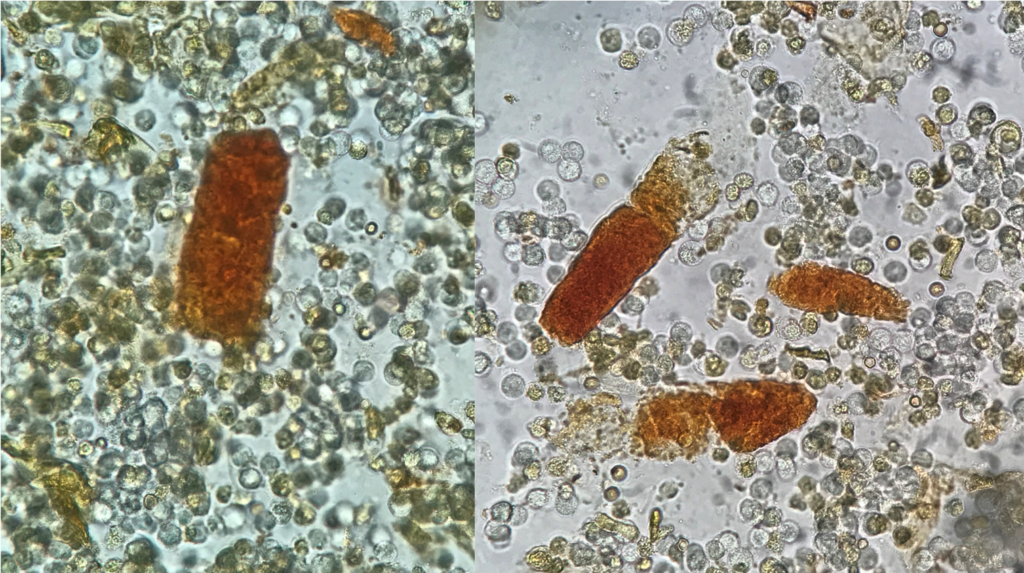
Myoglobin casts (Figures 5 and 6) have a reddish brown color, but are usually not associated with red blood cells or erythrocytic casts. They can be observed in the urine of patients with acute kidney injury (AKI) associated with severe muscle damage leading to rhabdomyolysis [6,7]. The main pathophysiologic mechanisms of AKI in this clinical setting are kidney vasoconstriction, direct heme-protein induced cytotoxicity, and intraluminal myoglobin cast formation.
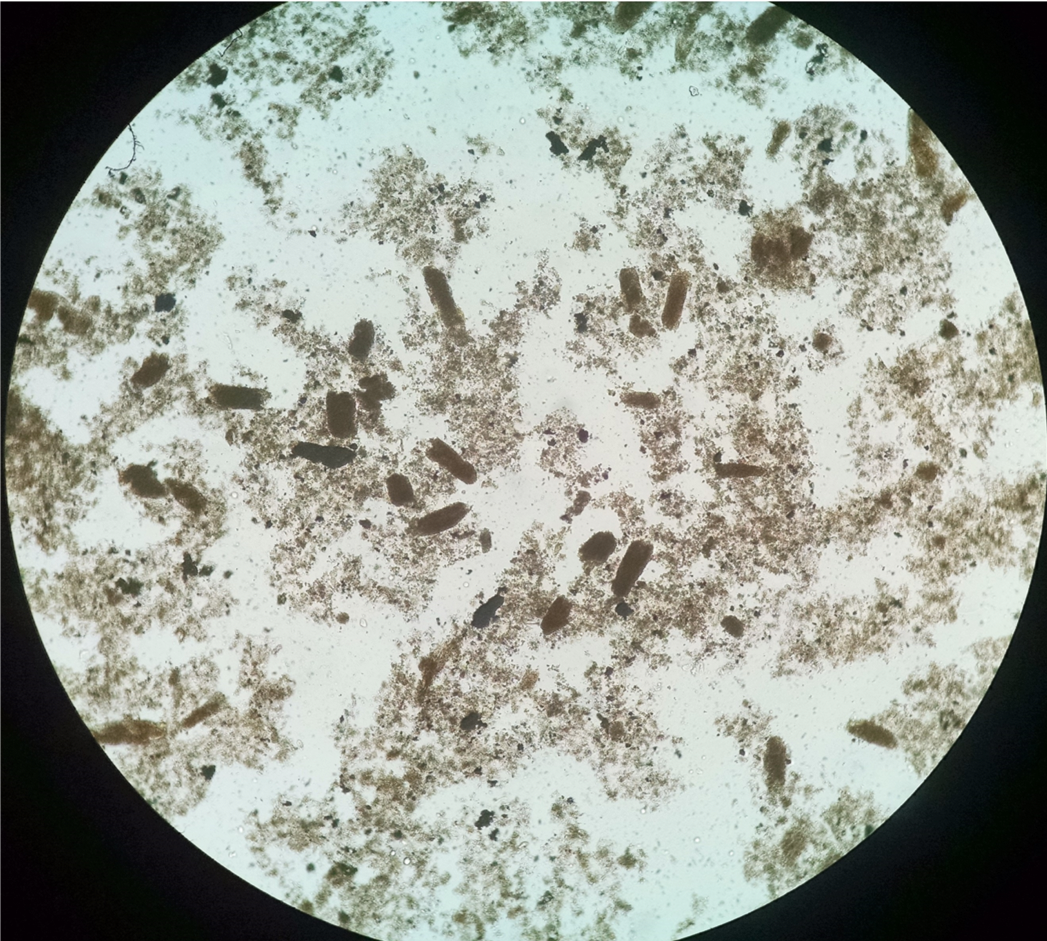
Kidney vasoconstriction occurs due to nitric oxide scavenging by heme proteins. Degradation of intratubular myoglobin results in the release of free iron, which catalyzes free radical production and further enhances ischemic damage. In addition, the heme center of myoglobin will initiate lipid peroxidation and kidney injury. The high filtered myoglobin load combined with low fluid flow rates predispose to obstructive cast formation within the distal tubules. A less recognized complication of rhabdomyolysis, which may also contribute to AKI, is hyperuricosuria and urate/uric acid crystal cast formation (Figure 6). High generation rates and urinary excretion of uric acid further contribute to tubular obstruction by urate/uric acid casts. Uric acid precipitation is also enhanced by low urine pH, which is frequently present in rhabomyolysis-associated AKI [8].
Hemoglobin Casts
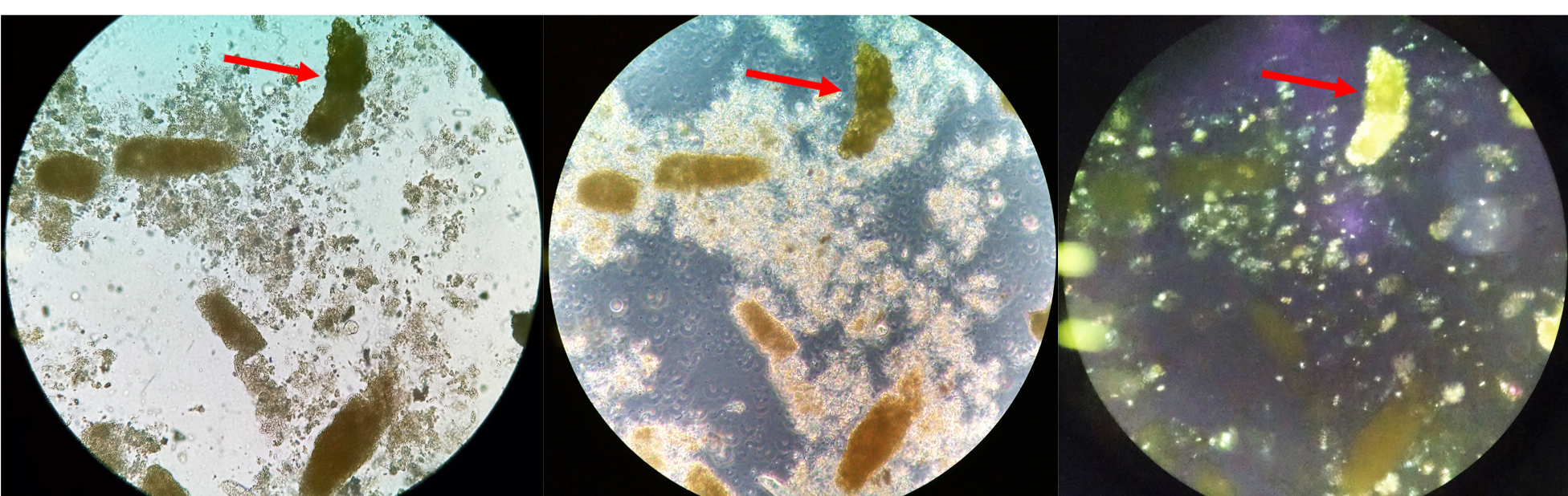
Hemoglobin casts originate from erythrocytes (Figure 7), have a typical hue that varies between brown and red, and often have a granular aspect. They are usually found in association with free red blood cells and erythrocytic casts in patients with kidney bleeding from various causes. The identification of this type of cast can be performed using the microadjustment of the microscope very carefully, which makes visualization of the membrane of remnant erythrocytes. possible Urine microscopy should also reveal features of glomerular hematuria.
In rare instances, hemoglobin casts are due to hemoglobinuria (Figure 8) and may occur in disorders associated with intravascular hemolysis [6,7]. In these cases, erythrocytes will not be observed or will be observed in very small numbers, despite the positive reading of “blood” on the urinalysis dipstick.
Hemoglobin casts (due to hemoglobinuria) and myoglobin casts are very difficult to differentiate – as both may cause tubular necrosis. To be able to properly differentiate these types of pigmented casts, the clinical history is key [7].
Bilirubin/Bile Casts
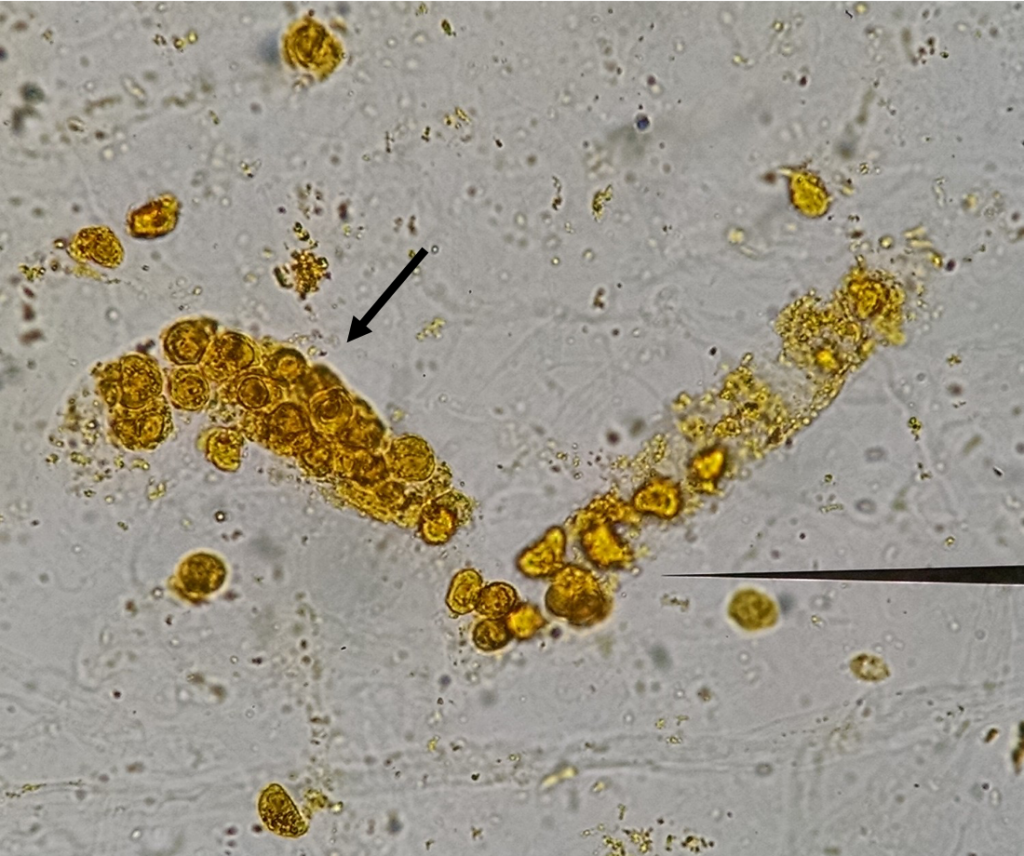
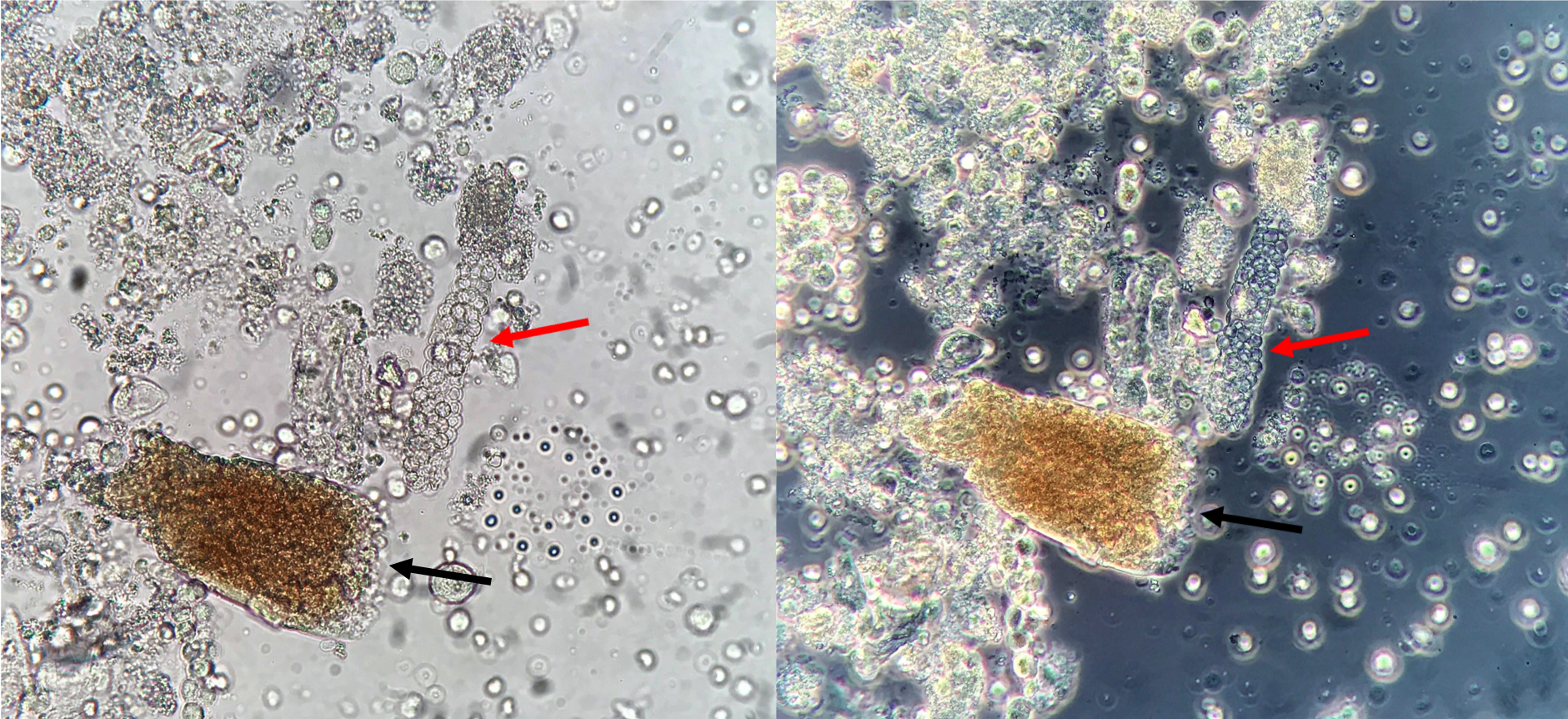
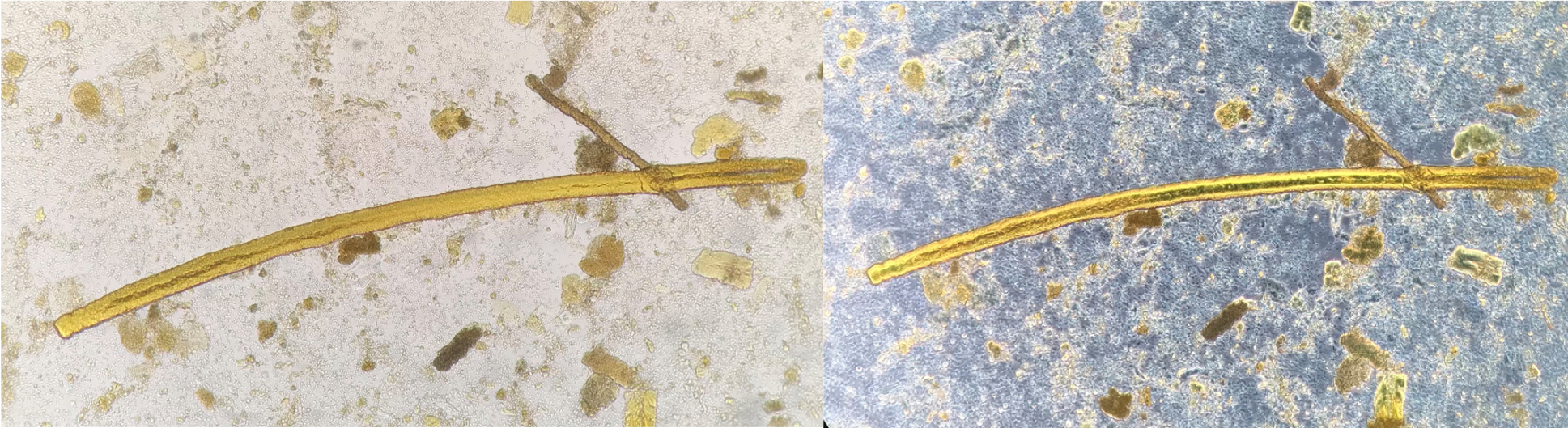
Bilirubin/bile casts (Figure 9) typically display the yellow-brown hue of bilirubin. In patients with underlying liver disease and elevated direct (conjugated) bilirubin, urinary casts may be stained yellow. A bilirubin-stained cast may be evidence of tubular injury. The mechanism of tubular injury in these cases is complex and not completely understood [7,9]. Usually, bilirubin/bile casts are observed as granular casts (Figure 10) or RTEC casts (Figure 11) – though casts with a waxy matrix (Figure 12) may also be similarly stained.
Phenazopyridine Casts
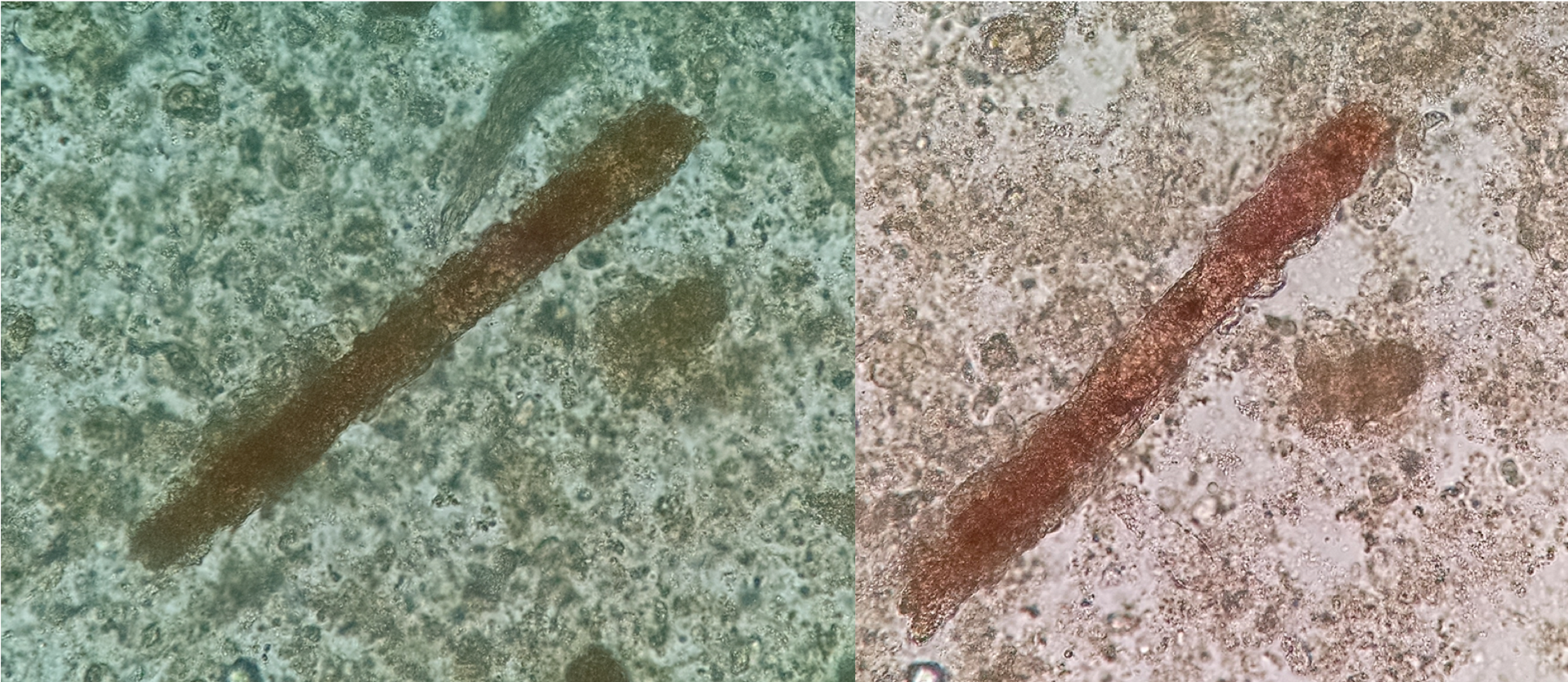
Phenazopyridine is the active compound in medications commonly for its anesthetic properties in patients with urinary tract infection symptoms. Metabolization of this drug produces an orange discoloration in the urine and high doses of this medication can cause AKI. In the setting of phenazopyridine-asscoiated AKI, phenazopyridine and granular casts (Figure 13) containing RTECs (Figure 14) can be observed [7].

In summary, a wide range of pigmented casts can be found in urine sediment specimens. The proper knowledge of their morphology and subtypes associated with the clinical information about the case may contribute to the correct diagnosis of kidney diseases.
Post by: José Antonio Tesser Poloni
References:
- Bywaters EG, Beall D. Crush Injuries with Impairment of Renal Function. Br Med J. 1941 Mar 22;1(4185):427-32.
- Beall D, Bywaters EG, Belsey RH, Miles JA. Crush Injury with Renal Failure. Br Med J. 1941 Mar 22;1(4185):432-4.
- Almond M. Professor Eric G.L. Bywaters, Acute Kidney Injury and the “forgotten” letter. G Ital Nefrol. 2016 Feb;33 Suppl 66:33.S66.9.
- Fogazzi GB. The Urinary Sediment, 3rd edition. Milano: Elsevier; 2010.
- Brunzel, Nancy A, Fundamentals of Urine & Body Fluid Analysis. St. Louis, Mo.: Elsevier/Saunders, 2013.
- Caleffi A, Lippi G. Cylindruria. Clin Chem Lab Med. 2015 Nov;53 Suppl 2:s1471-7.
- Recomendações da Sociedade Brasileira de Patologia Clínica/Medicina Laboratorial (SBPC/ML): Realização de exames em urina. 1ª edição, Editora Manole, Barueri/SP – Brazil, 2017.
- Tesser Poloni JA, Perazella MA. A Rarely Recognized Cause of Acute Kidney Injury in Rhabdomyolysis. Am J Med Sci. 2018 Sep;356(3):e27.
- Poloni JAT, Perazella MA, Keitel E, Marroni CA, Leite SB, Rotta LN. Utility of a urine sediment score in hyperbilirubinemia/hyperbilirubinuria. Clin Nephrol. 2019 Sep;92(3):141-150.