Subxiphoid, also known as the subcostal view is the easiest cardiac view to obtain in most patients. It is particularly useful in mechanically ventilated patients, as it can be obtained reliably when no other sonographic windows are found (parasternal views are often obscured by the distended lung). For point of care purposes, we can obtain most information seen on other cardiac views from the subxiphoid view. While performing cardiopulmonary resuscitation, this is a good view to evaluate the heart without interrupting the chest compressions. In nephrology practice, this is a reliable view to quickly exclude significant pericardial effusion.
Image acquisition:
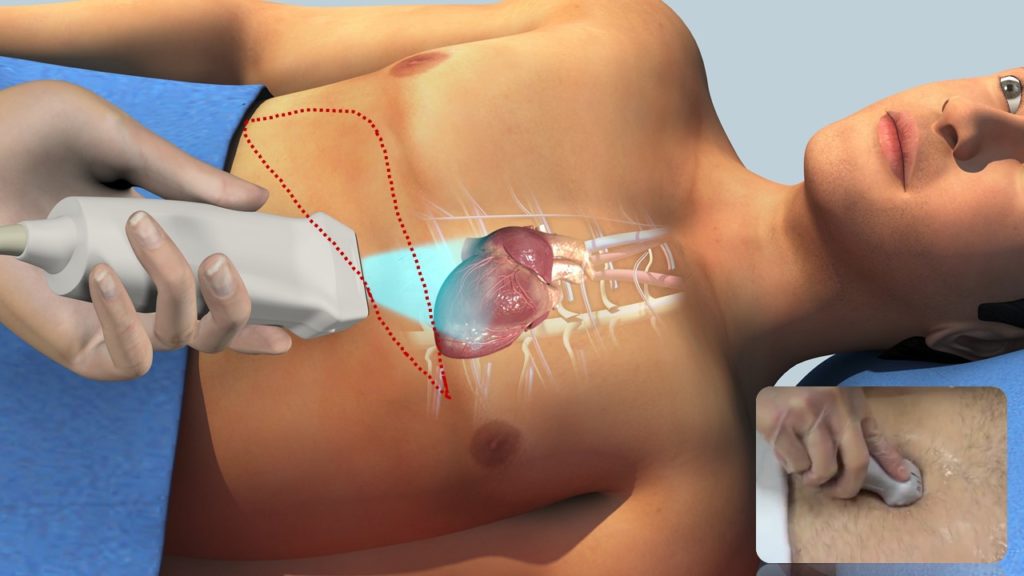
To obtain images from the subxiphoid window, the patient should be positioned supine with knees bent when possible to relax the abdominal wall musculature. As you may recall, this is different from the other cardiac views we have previously discussed, where a left lateral decubitus position helps to acquire optimal images. The probe is placed 2-3 cm below the xiphoid process and its face is directed upwards (= we are looking from abdomen into the chest) with the orientation marker pointing to patient’s left (3 o’clock). You may need to push the probe into the body slightly as shown in the inset of Figure 1 to get a better view and ask the patient to take a deep breath whenever possible. If you do not have a phased array probe (= cardiac probe) and the patient’s body habitus permits, a curvilinear probe (= abdominal probe) can be used to obtain this view but the image quality might not be adequate.
Sonographic anatomy:
The optimal view demonstrates all four chambers of the heart (= subcostal four-chamber view) with liver on top of the image (we are looking at the heart through the liver). Essentially, it looks like a tilted apical four-chamber view attached to the liver [Figure 2]. The right sided chambers are close to the liver. Though subxiphoid view looks like the apical four-chamber, it grossly underestimates the overall size (volume) of the ventricles. Having said that, right ventricular diastolic wall thickness is best assessed in this view because it is perpendicular to the beam of ultrasound (this is the ideal angle in greyscale ultrasound). For the same reason, this is a good view to assess atrial septal defects.
Other views and structures:
Gentle probe movements in the subxiphoid window allow us to visualize other structures in addition to coronal view of the heart.
By rotating the probe counterclockwise, we can obtain subcostal short-axis view [Figure 3], which is similar to the PSAX view. This allows measurements of left ventricular wall thickness and dimensions that are comparable with PSAX, although at a greater depth and through different myocardial segments. It is particularly helpful when parasternal window is inadequate because of inflated lungs or thoracic surgery.
Rotating the probe 90o counterclockwise from the four-chamber view trying not to lose the right atrium on the screen yields long axis view of the inferior vena cava (IVC) [Figure 4]. It is important to see the IVC-right atrial junction so that it is not mistaken for the aorta. As we know, evaluation of the size and respiratory variation of the IVC aids in volume status assessment when interpreted in the right clinical context.
We can also see the short axis view of the IVC and the hepatic veins draining into it by tilting or fanning the probe slightly down from the four-chamber view [Figure 5]. This venous confluence is compared to moose head or stag head, especially when they are dilated in the setting of congestive heart failure.
If you are confused about the terminology of the probe movements, watch this short video.
Now we will briefly discuss some of the common abnormalities seen in this view pertinent to nephrology practice. Pearls and pitfalls of IVC POCUS will be discussed in a separate post.
Pericardial effusion:
As mentioned before, pericardial effusion appears as an anechoic or echo-free space between the two layers of the pericardium. In subxiphoid view, an effusion can easily be seen in the space between the liver and the right ventricle. Due to liver tissue’s homogeneity and inherently high propagation speed of sound waves, it serves as an excellent acoustic window to detect pericardial effusion. As a reminder, we are looking at the heart through the liver in this view. Make sure to rock and fan the probe gently to visualize the entire area surrounding the heart so that small localized effusions are not missed.
Following image [Figure 6] was obtained from an end stage renal disease patient with significant hypervolemia. Note moderate to severe pericardial effusion, which improved with aggressive ultrafiltration.
Pleural effusion:
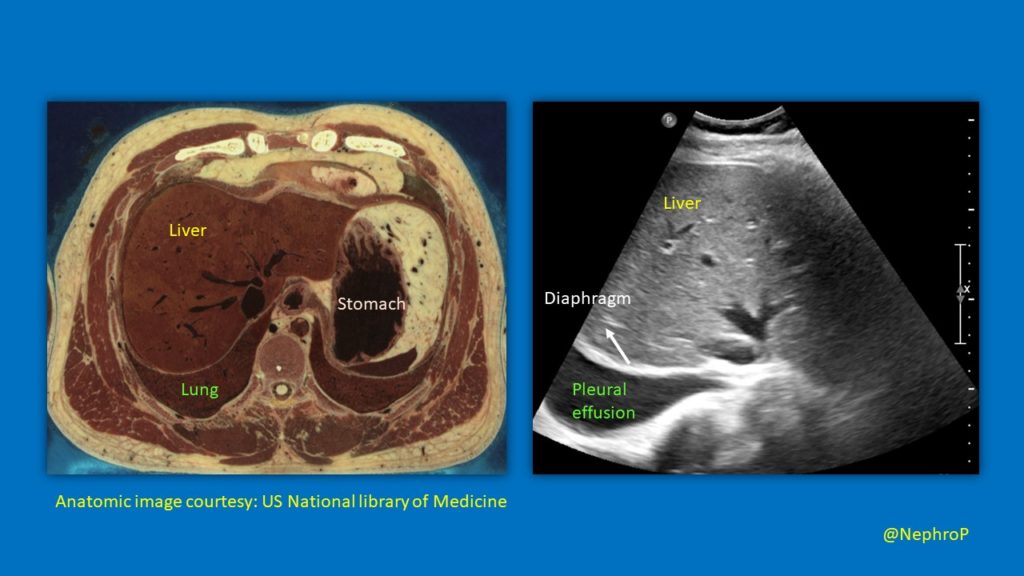
We know that pleural effusion is usually evaluated in the mid-axillary plane. However, it is interesting to note that pleural effusion (particularly right) can be seen on subxiphoid scans in transverse/oblique plane. Following anatomic correlate [Figure 7] illustrates this better.
Here is a nice image [Figure 8] demonstrating right pleural effusion, inferior vena cava and the heart from the subxiphoid window.
Below is the stag head sign in a patient with congestive heart failure [Figure 9]. As mentioned above, it represents dilated IVC and hepatic veins in the transverse plane. Additionally, note the right pleural effusion.

Atrial swirl sign:
Subxiphoid four-chamber view can also be used to confirm the appropriate placement of central venous catheter by eliciting the rapid atrial swirl sign. Refer to the post on apical four-chamber view for further description of this sign.
Abhilash Koratala MD
@NephroP

1 comment