Our focus on myeloma related disorders continues- view previous posts here.
Pathogenesis
Proliferative glomerulonephritis with monoclonal immunoglobulin deposition (PGNMID) is seen in less than 1% of native kidneys and is due to IgG kappa (IgG3 most commonly) deposition in the glomeruli. IgG3 is nephritogenic and highly complement fixing.
Clinical presentation
Patients have an average age of 55 years (range: 7-81 years old) and PGNMID more commonly affect females (2:1). These patients often present with nephrotic range proteinuria (70%) and hematuria. There is a rare association with multiple myeloma and a bone marrow biopsy is necessary to rule out a plasma cell neoplasm. Approximately 30% of patients will have serum or urine monoclonal proteins. A quarter of the cases will have low levels of C3 and C4. Recurrence rate amongst allografts is high.
Light microscopy
Patterns of injury include membranoproliferative (57%), endocapillary proliferative (35%), membranous (5%) and mesangial proliferative (3%).
In the most common pattern, membranoproliferative, frequent glomerular basement membrane duplication with mesangial hypercellularity and matrix expansion is seen (Figure 1 & 2). Approximately 30% of mesangial proliferative cases can show crescent formation.


Immunofluorescence microscopy
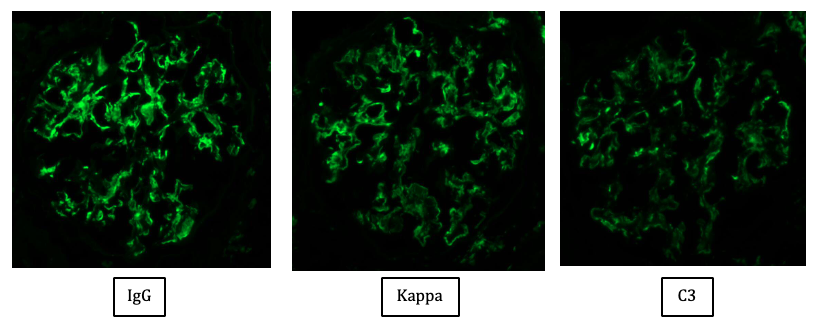
Coarsely granular mesangial and capillary wall staining with IgG (IgG3 most common sub-class followed by IgG1) is seen. Kappa light chain restriction is more common (73%). C3 staining is frequently present with C1q staining in 60%. In cases with a membranous pattern, there is finely granular capillary wall staining. No staining is present outside the glomeruli (Figure 3).
Electron microscopy
EM findings are typical for unorganized mesangial and subendothelial amorphous electron dense deposits. In the membranous pattern of injury, occasional subepithelial deposits are also present (Figure 4 & 5).


Treatment
Patients with PGNMID can be treated with steroids alone or with immunosuppressive agents such as rituximab or cyclophosphamide.
Prognosis
Forty percent of patients show partial or complete recovery and approximately 20% progress to end stage renal disease. Poor prognostic indicators are high serum creatinine at presentation and severity of glomerulosclerosis and interstitial fibrosis.
Differential Diagnoses
Lupus nephritis: Cases will also stain with C1q however; there will be no light chain restriction.
Membranous glomerulonephritis: Deposits will stain for both kappa and lambda light chains.
Membranoproliferative glomerulonephritis: Deposits will stain for both kappa and lambda light chains.
Type 1 Cryoglobulinemic glomerulonephritis: Type 1 cases are usually IgG3 (similar to PGNMID). Light microscopy can show intraluminal pseudothrombi in the glomeruli and there will be a positive test for cryoglobulinemia.
Light and heavy chain deposition disease: Nodular sclerosing glomerulopathy by light microscopy. EM findings will show powdery electron dense deposits not only in the glomerular basement membranes but the tubular basement membranes as well. PGNMID will not show any extraglomerular deposits.
Membranous like glomerulonephritis with masked IgG kappa deposits: Patients with this entity are commonly women in their mid 20s who have autoimmune phenomena.
Tripti Kumar, DO
Renal Pathology Fellow
University of Chicago