Cystinuria is the most common kidney stone disease with Mendelian genetics. Caused by mutations in SLC7A9 and SLC3A1, affected patients excrete high amounts of cystine in their urine and are vexed by recurrent episodes of nephrolithiasis.
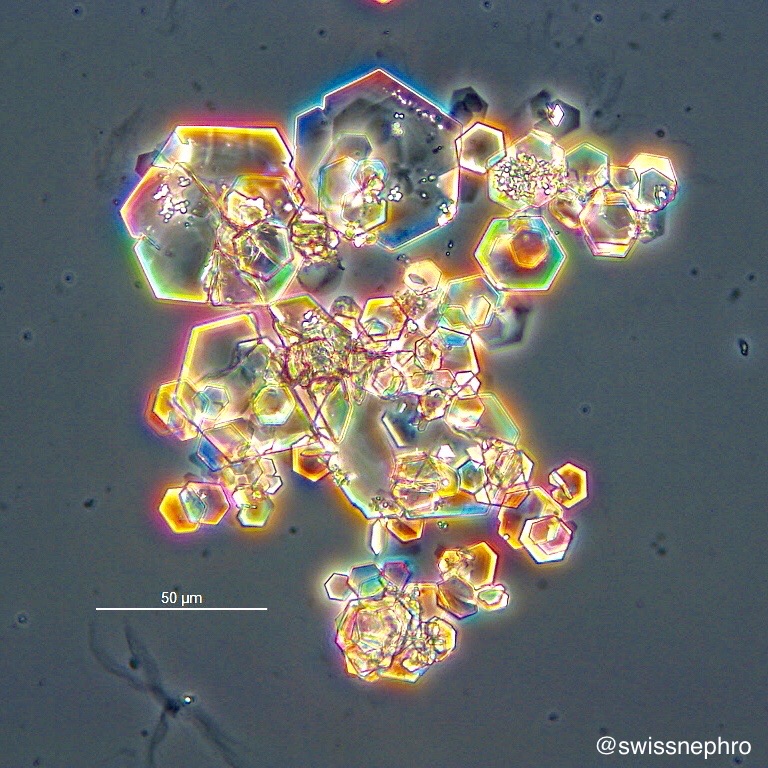
Cystine stones (Fig. 1) are aggregates of individual crystals with hexagonal habits. In the urinary sediment pathognomonic hexagonal plates with large basal surfaces can be found (Fig. 2).

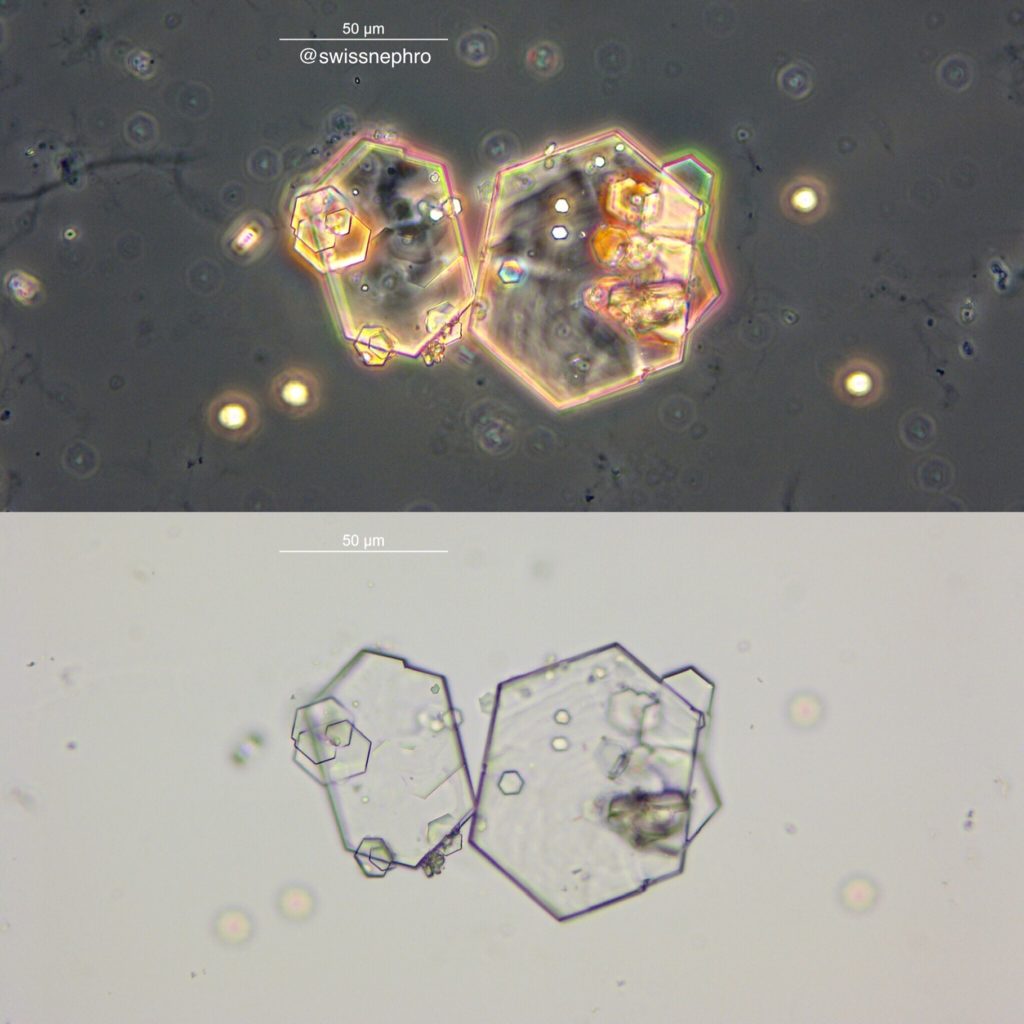
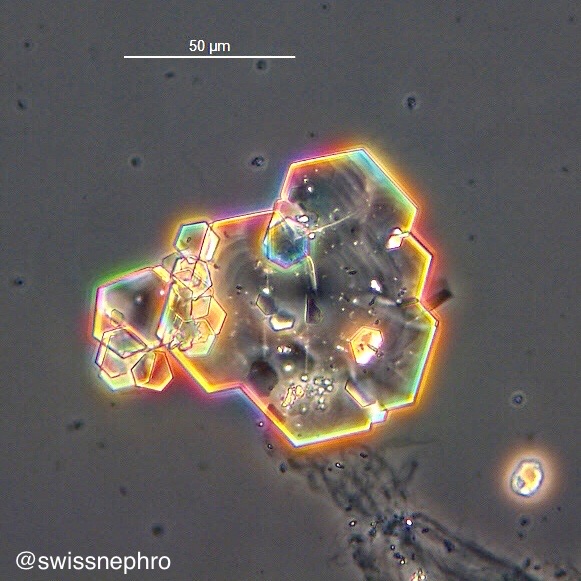
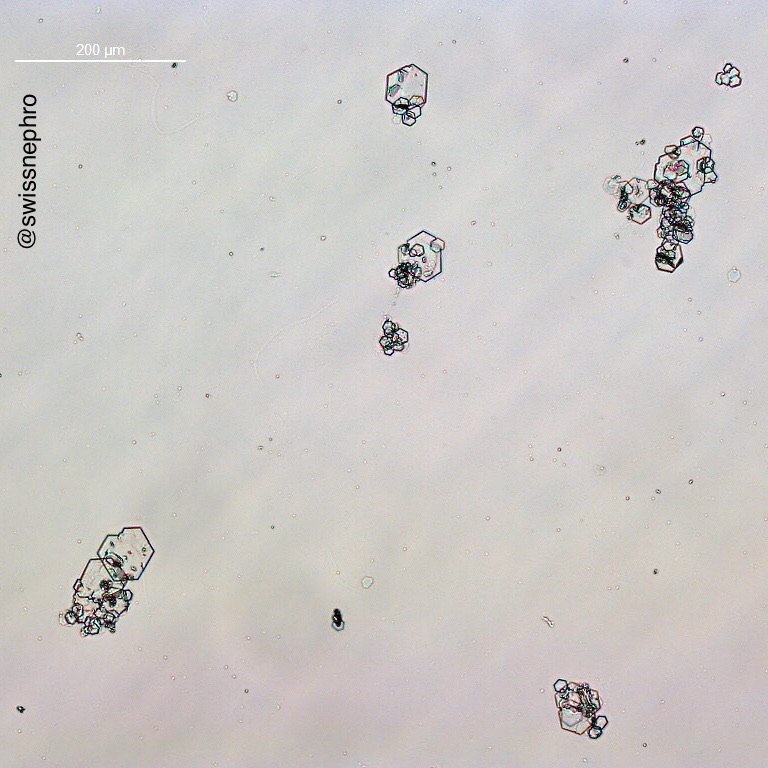
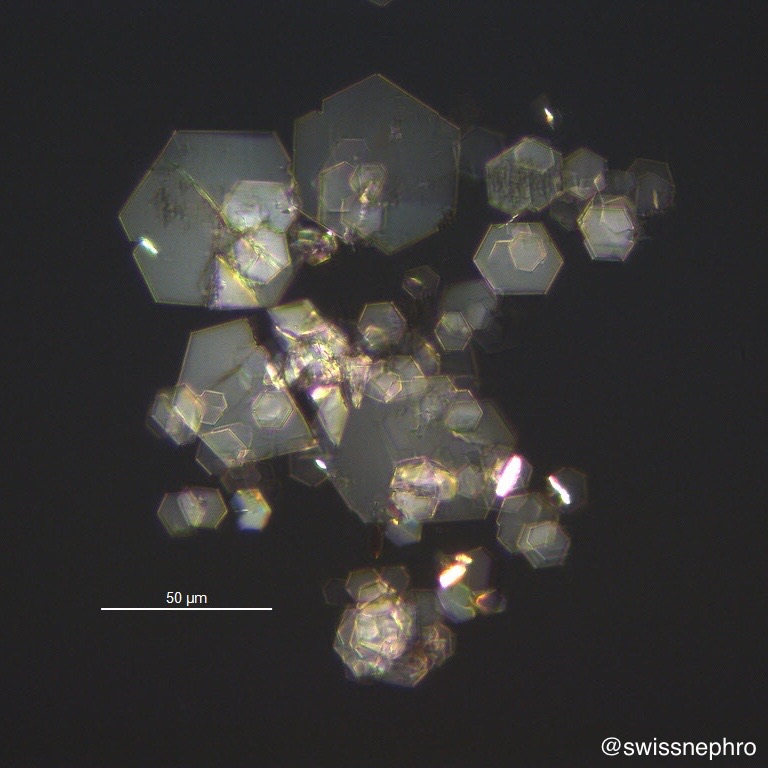
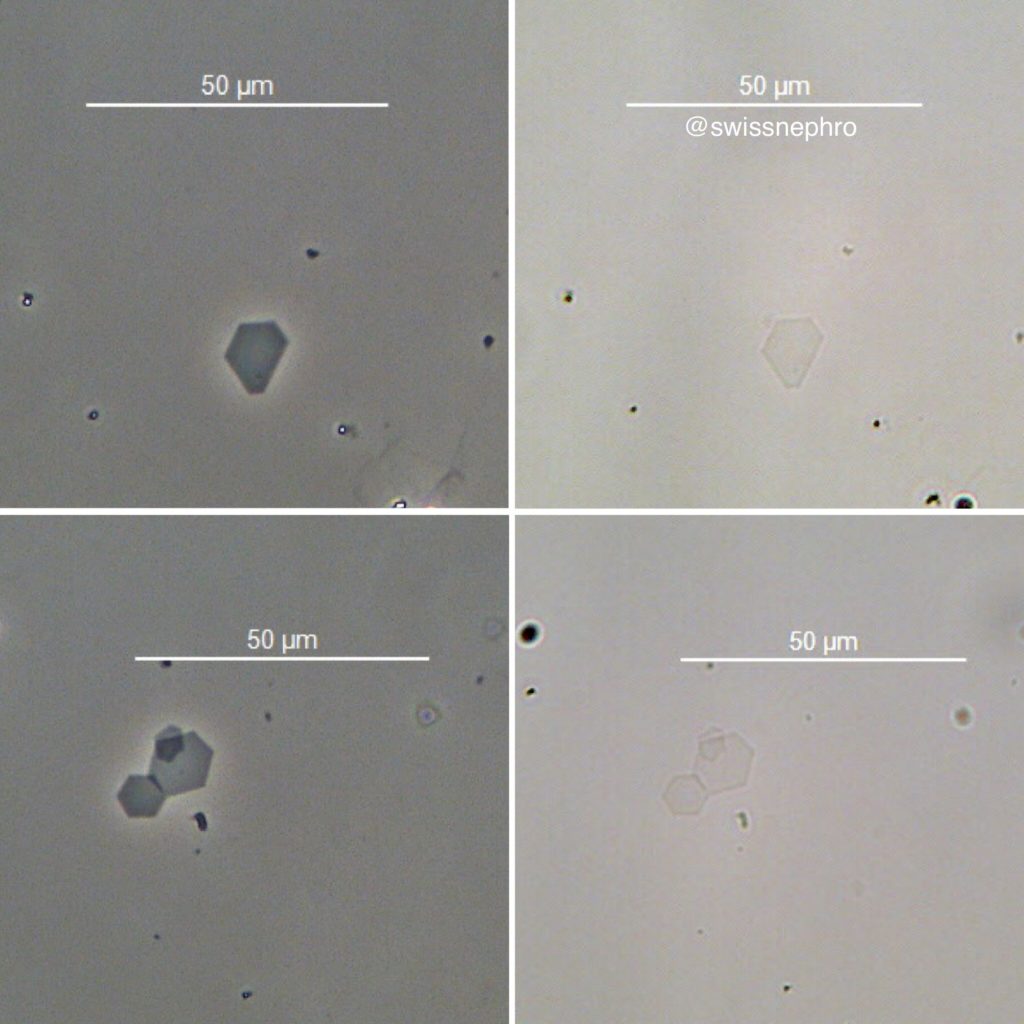
Although cystine crystals in the urine may form complex aggregates (Fig. 3 and 4), the underlying hexagonal structure is usually readily discernible. Characteristically, they are colorless with bright field microscopy and the crystal margins are perfectly linear (Fig. 5). Phase contrast might create some color artifacts (Fig. 6 and 7).
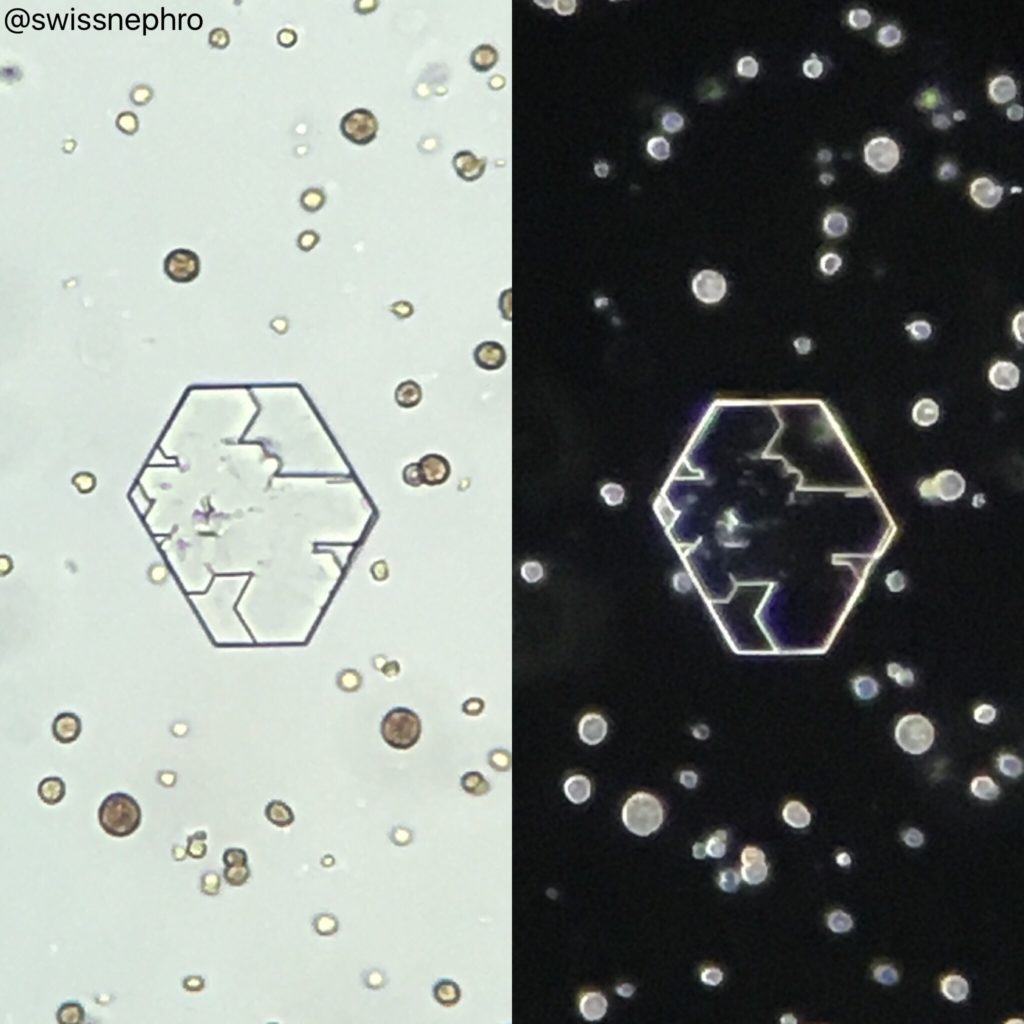
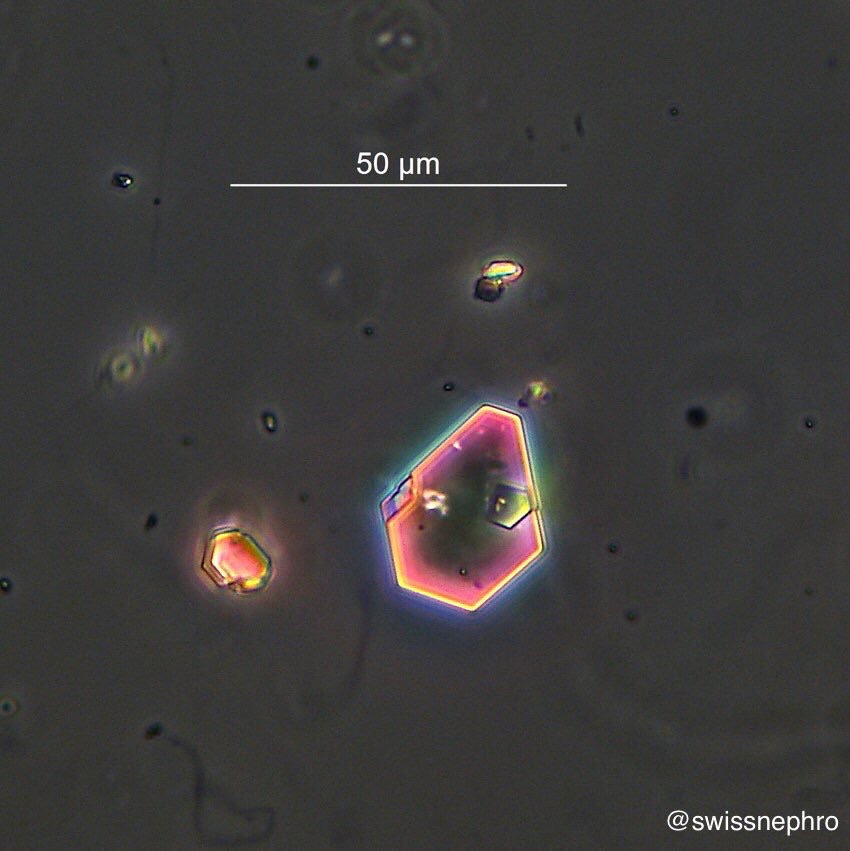
Depending on the thickness of the crystals, their birefringence tends to be of low to moderate intensity (Fig. 8). Very thin crystals are easily missed, especially by bright field microscopy alone (Fig. 9).
Cystine crystals in the urinary sediment (a) confirm the presence of cystinuria and (b) demonstrate urinary supersaturation of cystine.
While perfectly specific, the sensitivity of cystine crystalluria for the presence of cystinuria is quite low.
Post by: Florian Buchkremer

