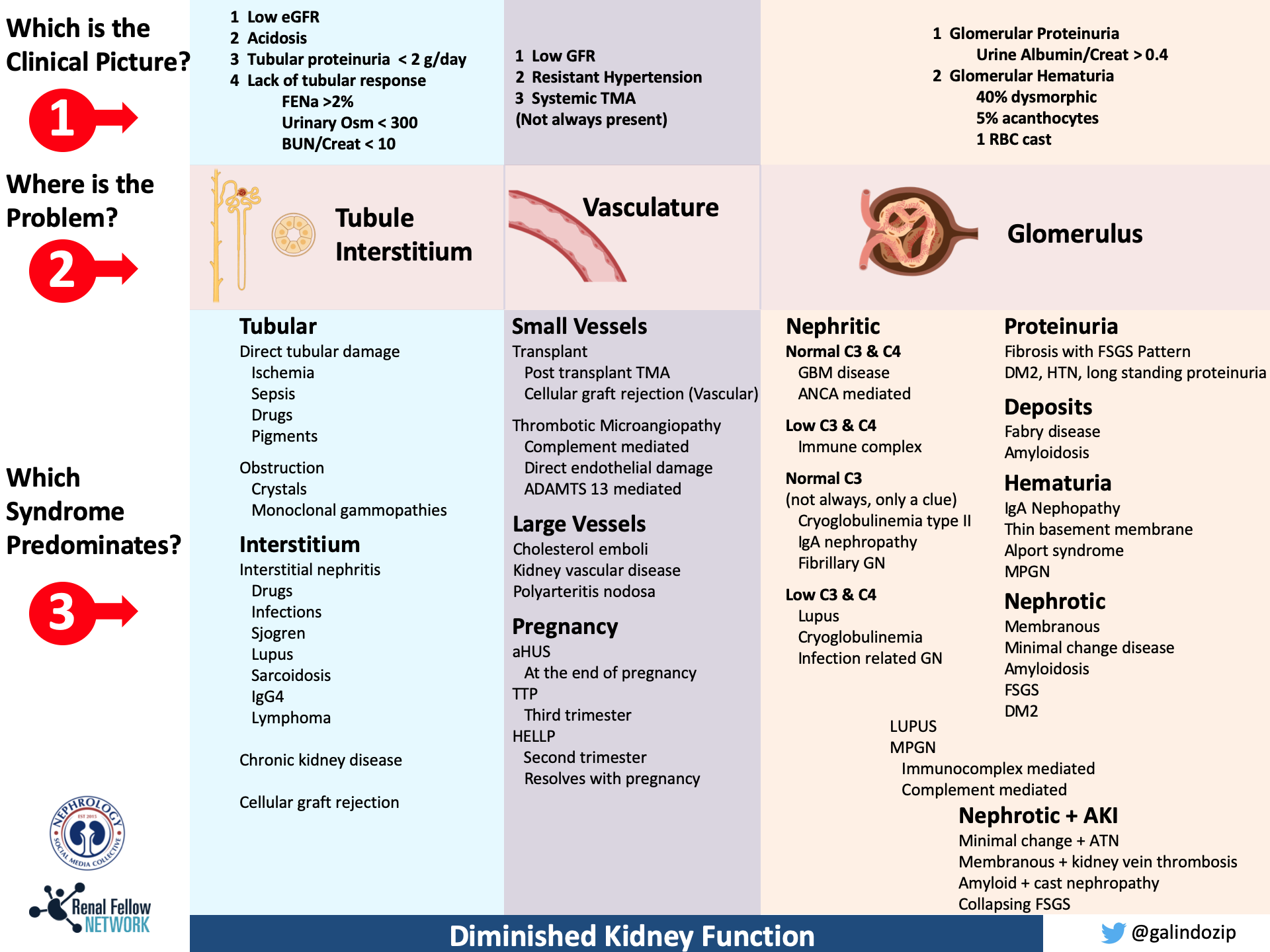
Whenever there is a diagnostic problem in nephrology we traditionally try to integrate syndromes and generate a list of differential diagnoses. This can help us focus a workup and sometimes even start treatment before a biopsy is reported. When I was a first year nephrology fellow, I found it very complicated to use the traditional syndromes (nephrotic, nephritic, CKD, AKI) to come with differential diagnosis during clinical- pathological conferences. This is because many of the syndromes overlap. Moreover, the syndromes are typically taught as discreet entities. That’s where I noticed that several of the other fellows had experienced an attending who used a different way. In this approach, you initially try to figure out what was the clinical picture that predominates. This clinical picture is used to help localize the lesion in the kidney (just like neurologists localize to the lesion in the nervous system with their physical exam). After localizing the problem it was much easier to direct the work up and find the more probable differentials. I realized that a useful way to divide the many different kidney diseases was to localize the problem into three different sections of the kidney:
- Tubule and interstitium
- Vasculature
- Glomerulus.
Each of them with a particular classical clinical presentation that I called “the kidney syndromes”: tubule/interstitial syndromes, vasculature syndromes and the already existent glomerular syndromes. With this in mind I designed a visual box with the most common and exclusive clinical characteristics of each kidney section and with possible differentials according to directed workup. The table has three sections that follow the definition of a syndrome: 1 signs and symptoms, 2 some pathophysiology (location of problem) and 3 different causes. I found it very accurate during clinical- pathological sessions and definitely guided the way I think of nephrology diagnostic problems in practice. The approach is not free of error or controversy and should only work for guidance and diagnostic order.
Pablo Galindo, MD
Nephrologist, Mexico City, Mexico
NSMC Intern 2020
@galindozip
Very helpful
Compact and informative. Thank you.
Dr Galindo. Thank you for sharing your approach to renal disease. It is always refreshing to have a new perspective on a subject that has always been taught the same way.
I noticed in your nephritic group, you have Low C3 and C4 repeated twice as a section. Can you please enlighten us about that?
Dr. Galindo,
The Kidney Syndromes-picture guide is very helpful. Thank you!
It is on the post
Where’s the table