Microscopic examination of the urinary sediment in the context of hyperbilirubinemia and increased urinary bilirubin excretion requires special attention to the unique chromatic characteristics acquired by the specimens. As serum bilirubin increases, a yellow-tinged urine becomes increasingly noticeable. This is notorious in patients with serum total bilirubin approximately greater than 20 – 30 mg/dL.
Cirrhosis, obstructive or drug-induced cholestasis, and alcoholic hepatitis represent the most important categories of patients with this feature. When patients with those entities present with acute kidney injury (AKI), careful inspection of the urinary sediment is required to assess for evidence of acute tubular injury or other parenchymal cause of AKI. Urine sediment can help make a diagnosis of hepatorenal syndrome type 1 or entertain others such as cholemic nephrosis.
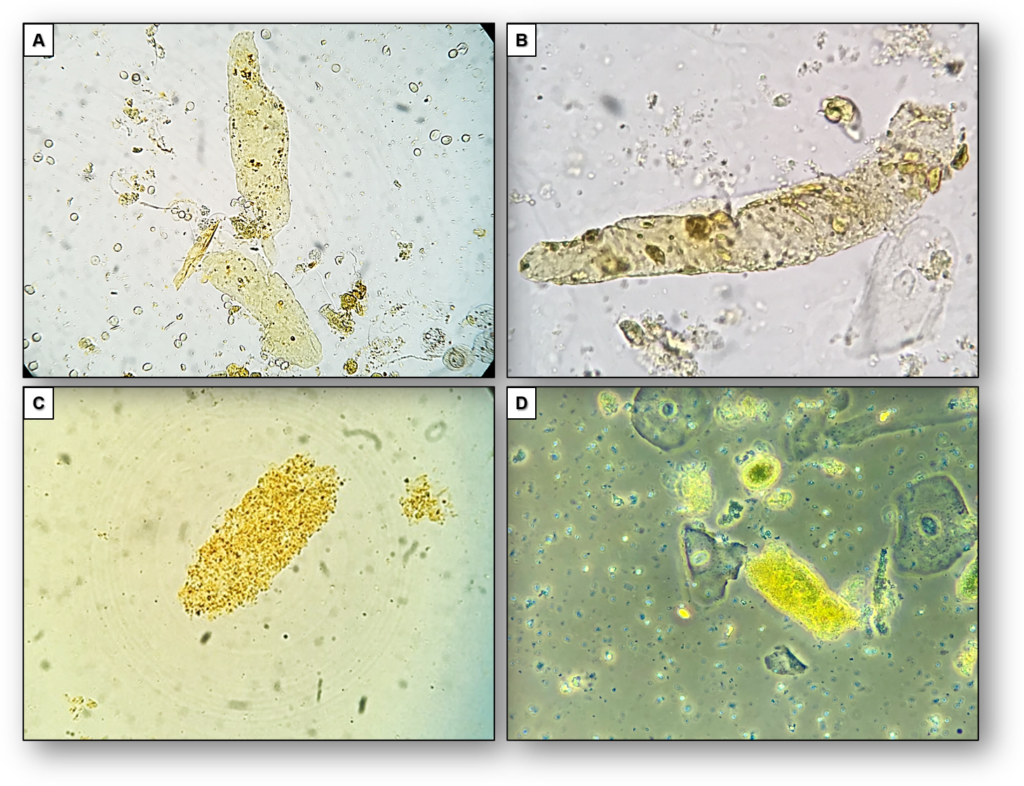
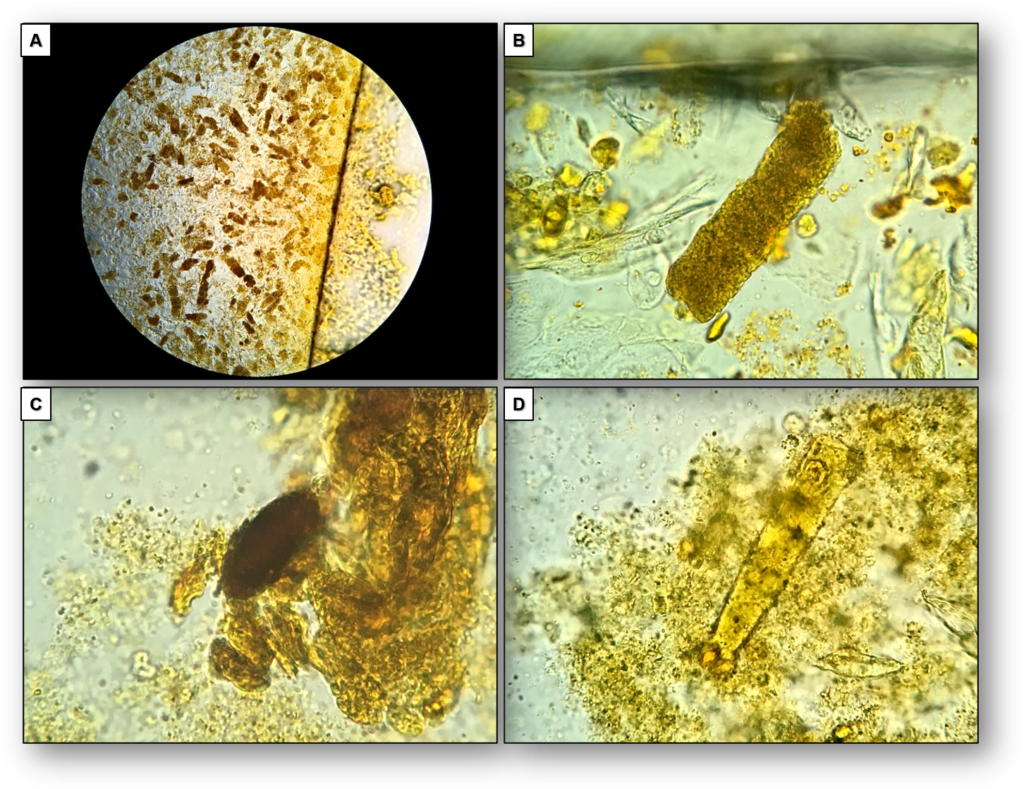
Because of staining by bilirubin, hyaline casts may become more apparent (Figure 1) and granular and waxy casts may have various degrees of color intensity (Figures 1, 2). Use of Sternheimer-Malbin (SM) stain is usually not necessary in this context, but when it is used, the mixture of bilirubin and the violet color of SM stain creates a distinct orange/maroon color.
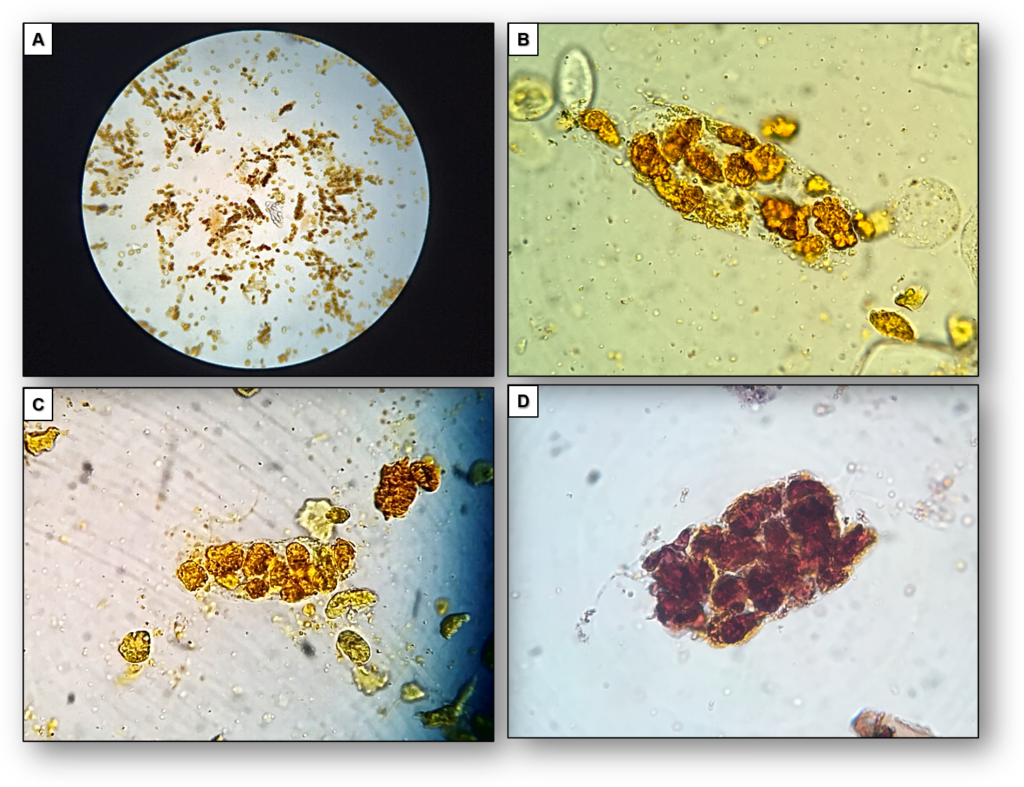
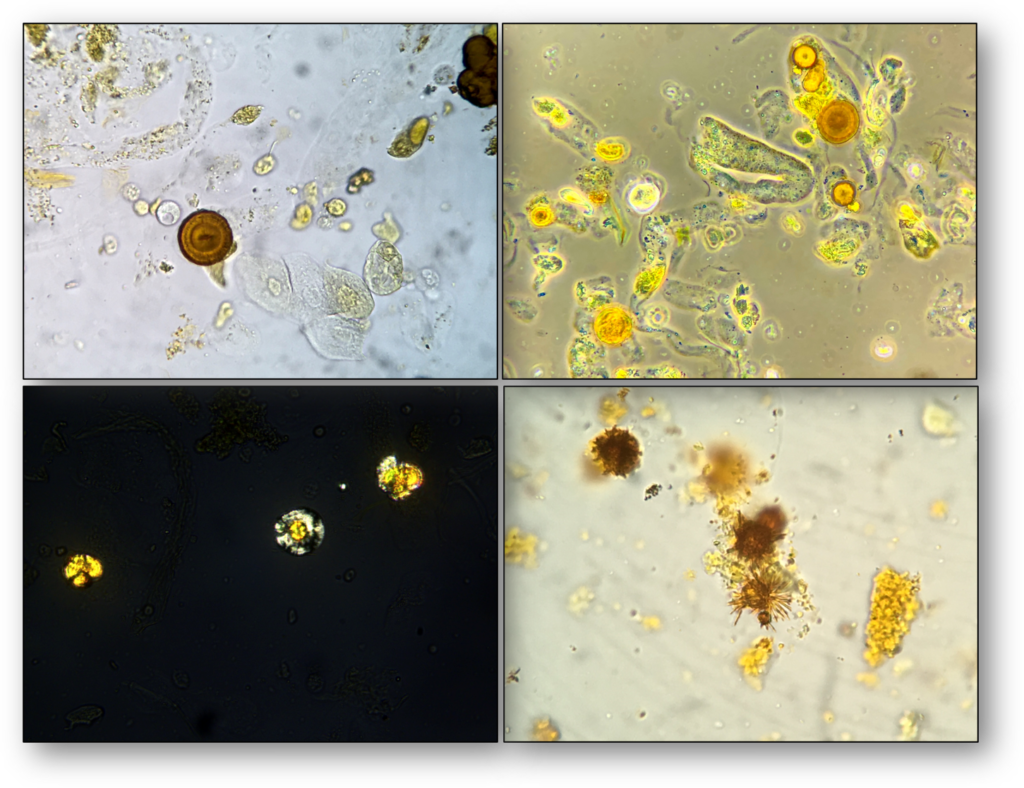
In patients with markedly elevated total bilirubin, renal tubular epithelial cells are a common finding (Figure 3), whereas leucine and bilirubin crystals can be identified only occasionally (Figure 4).
By Juan Carlos Velez @VelezNephHepato
#UrinarySediment #PisseProphet #UrineMicroscopy #SpinYourOwnUrine

Thank you so much!