Sodium-glucose co-transporter 2 inhibitors (SGLT2is) have emerged as a breakthrough therapy for the treatment of diabetes mellitus (DM) reducing key cardiovascular and kidney endpoints. These effects appear to be independent of their effects on blood pressure and glucose. However, every drug has side effects and SGLT2is have unique negative attributes that all clinicians should be aware of. In 2015, the FDA issued a warning regarding the risk of euglycemic diabetic ketoacidosis (EuDKA) with the use of SGLT2i.
EuDKA is characterized by metabolic acidosis and ketosis in the presence of normal or moderately increased blood glucose levels.In most cases, blood glucose values remain less than 250 mg/dl.
When we analyze it with the other side effects of SGLT2i, for example, chances of urosepsis (<1 in 500 patients), the occurrence of EuDKA with SGLT2i is an infrequent finding. With 100 mg and 300 mg of canagliflozin, incidence rates were reported as 0.52 and 0.76 per 1000 patient/yr respectively.
Euglycemic DKA versus DKA
As opposed to EuDKA (where blood glucose levels are normal or mildly elevated), typical DKA in Type 1 and 2 DM presents with marked hyperglycemia (usually 350–800 mg/dL) and associated with increased endogenous glucose production. Nevertheless, there is a reduction in tissue glucose disposal in the vicinity of insulin resistance. In EuDKA, insulin deficiency is milder and there is rather an improvement in insulin resistance.
| Euglycemic DKA | DKA | |
| Blood glucose levels | <250mg/dl | >250 mg/dL, typically 350–800 mg/dL |
| Symptoms | Mild or absent | Present |
| Insulin deficiency | ↑ | ↑↑ |
| Insulin resistance | ↓ | ↑↑ |
| Renal glucose clearance | ↑↑ | ↑ |
| Endogenous glucose production | ↑ | ↑↑ |
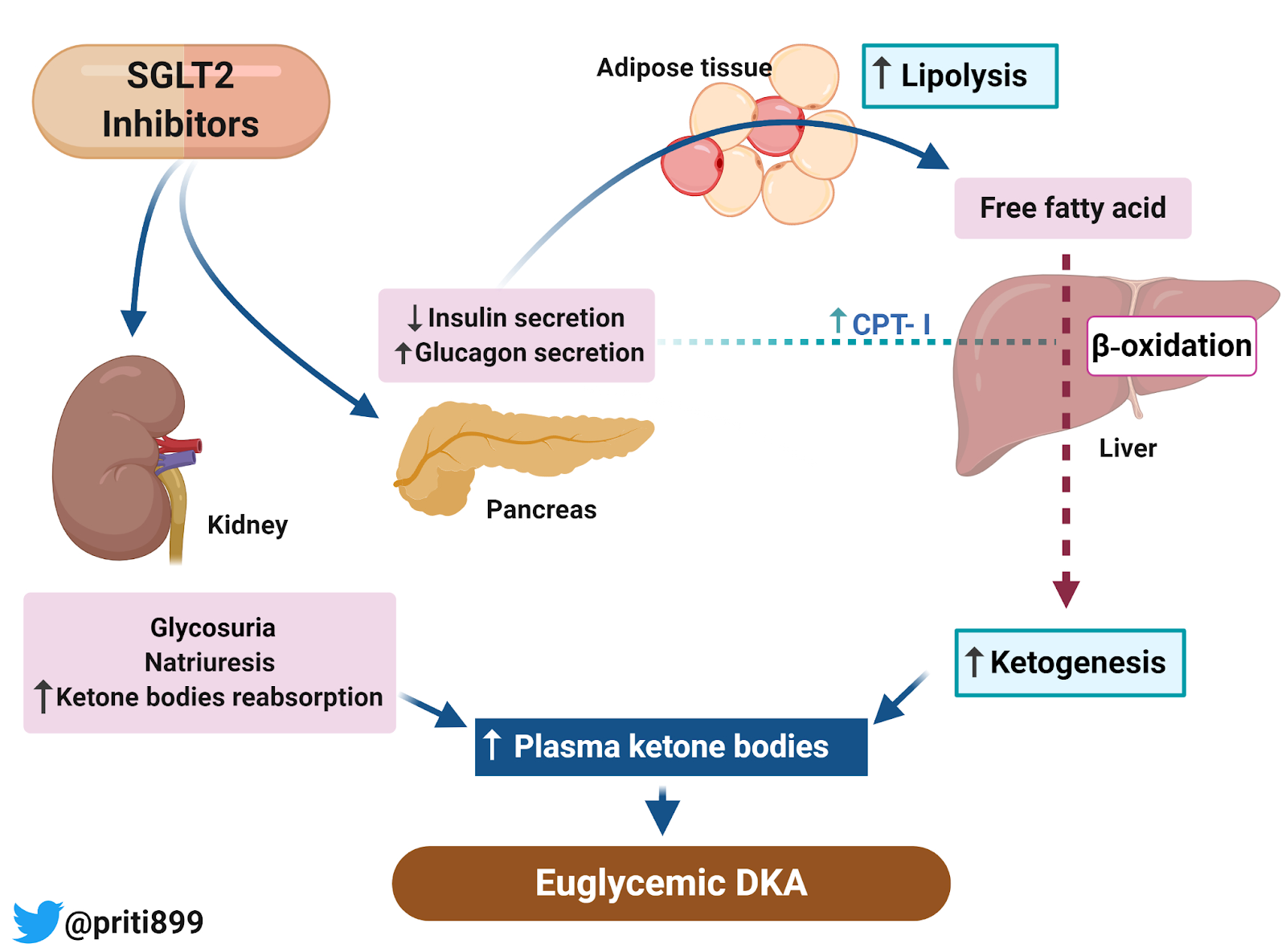
SGLT2is lowers blood glucose levels modestly by inhibiting glucose reabsorption in the proximal tubule leading to urinary glucose excretion. A decrease in blood glucose, in turn, reduces insulin secretion from β‐cells of the pancreas and stimulates the secretion of glucagon from pancreatic α‐cells. Consequently, increased glucagon‐to‐insulin ratio enhances gluconeogenesis along with lipolysis at the expense of carbohydrate oxidation which ultimately facilitates ketogenesis by shifting substrate usage from carbohydrates to lipids and ketone bodies. The reduction of antilipolytic activity of insulin triggers the production of free fatty acids (FFA), which are subsequently converted to ketone bodies via β‐oxidation in the liver. Furthermore, the decrease in insulin levels also promotes ketone bodies synthesis by activation of carnitine palmitoyltransferase–I (CPT‐I) which is responsible for the transport of FFA into mitochondria and hence increases the rate of β‐oxidation. In addition, the natriuresis and osmotic diuresis induced by SGLT2i may result in negative volume status.
The role of kidneys
The kidney tubules have a large capacity to reabsorb and use ketone bodies. The reabsorption of ketones in proximal tubules occurs via sodium-dependent monocarboxylate transporters (SMCT1 and SMCT2) which is dependent on sodium gradient (lumen to proximal tubule). Inhibition of SGLT2i may increase the sodium delivery to SMCTs thereby promoting ketone reabsorption.
In summary, SGLT2 inhibitors render the body susceptible to acidemia while producing glycosuria thereby causing near normal or less abnormally elevated glucose levels than conventional DKA.
At-risk patients
Fortunately, not all the patients taking SGLT2i’s develop EuDKA. In a majority of patients, it is precipitated by a reduction or discontinuation of insulin, following starvation or low carbohydrate diet, urosepsis, dehydration, severe acute illness, heavy physical exercise, or excessive alcohol intake. However in most cases, the triggering factor may not be identified.
Implications in clinical practice
The patient with EuDKA may not present with typical clinical signs and symptoms of DKA like dehydration because of the absence of marked hyperglycemia. Because of their atypical presentation, there is an increased probability of missing the diagnosis. Any diabetic patient taking SGLT2i presenting with symptoms like abdominal pain, nausea, vomiting, or fatigue should raise the suspicion of EuDKA. To diagnose EuDKA, keep in mind that the predominant ketone body is β-hydroxybutyrate i.e measured in blood, so measuring only urinary ketone body (acetoacetate ) may be deceiving as it is much less sensitive. Once the diagnosis is confirmed, it is advisable to stop SGLT2i immediately and manage the patient with hydration and insulin therapy, correction of electrolytes with the same protocol followed for DKA.
Priti Meena, MD
Nephrology Fellow, New Delhi
NSMC Intern 2020
@priti899
it is a stupid vision and a bad understanding of our body’s functionality SGLT2i are prone to induce ketosis.
ketone bodies are a better nutritional source of energy as shown by numerous studies that chack nutritional ketosis. stoping SGLT2i should be considered only in the setting of acidosis.
VERY NICE ARTICLE , WELL DONE
WELL DONE , VERY NICE ARTICLE . CLEAR IN ALL ASPECT INTRODUCTION, PATHOPHYSIOLOGY, DIAGRAM , EVERY BOARD MEDICAL RESIDENT
SHOULD RED IT , TO DIFFRENTIATE BETWEEN SERIOUS DKA AND EUG-DKA, RENAL FELLOW MUST
READ IT TOO.
Very nicely written n short & crisp. Thanx
Thankyou
Excellent article. Complex pathophysiology explained very well.Well done.
Very nicely written
Nice review.