Simon Smith, MD
Intern
Queen Elizabeth Hospital, Gateshead, UK
Jamie Willows, MD
Renal fellow
Freeman Hospital, Newcastle Upon Tyne, UK
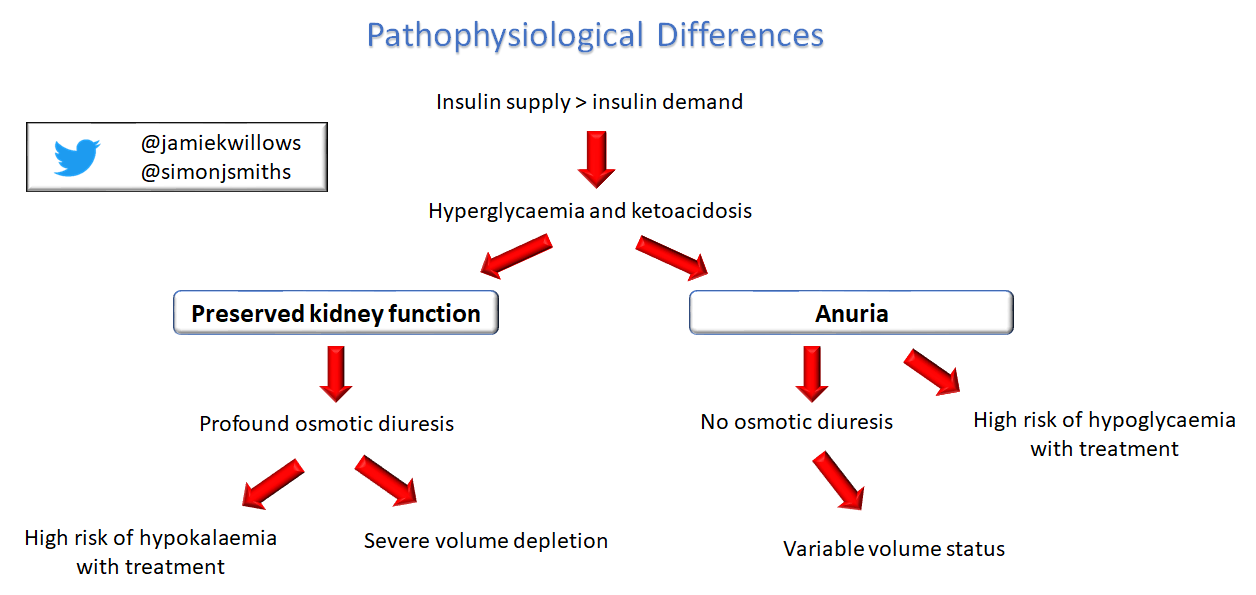
Diabetic ketoacidosis (DKA) is a well recognised complication of diabetes when insulin supply cannot meet demand. To briefly recap the familiar pathophysiology:
- Insulin Deficiency (or Loss) – Complete or relative insulin deficiency, along with a stress response and a rise in glucagon levels, leads to glycogenolysis and hyperglycemia
- Hyperosmolar State and hypovolemia – If you have preserved kidney function, this hyperglycemia causes a hyperosmolar state, and drives a profound osmotic diuresis. Patients are frequently 5-6 litres hypovolemic.
- Ketone Body Formation – Insulin deficiency also leads to lipolysis and the formation of ketone bodies, causing acidemia
- Hyperkalemia (with whole body potassium loss) – Patients often present with hyperkalemia due to a combination of insulin deficiency and solute drag from hypertonicity – however, the osmotic diuresis prior to admission will have caused electrolyte loss and rendered the patient whole body potassium deplete, and therefore they will rapidly develop need for potassium replacement once treated with insulin.
As DKA is a common but potentially life-threatening condition, many hospitals and health care systems recommend set protocols to guide practitioners through identification of the underlying cause and initial management with aggressive volume expansion, intravenous insulin, and electrolyte replacement. However, DKA management is very different in patients who lack kidney function and are on dialysis.
What is different in the patient with anuria who doesn’t undergo osmotic diuresis?
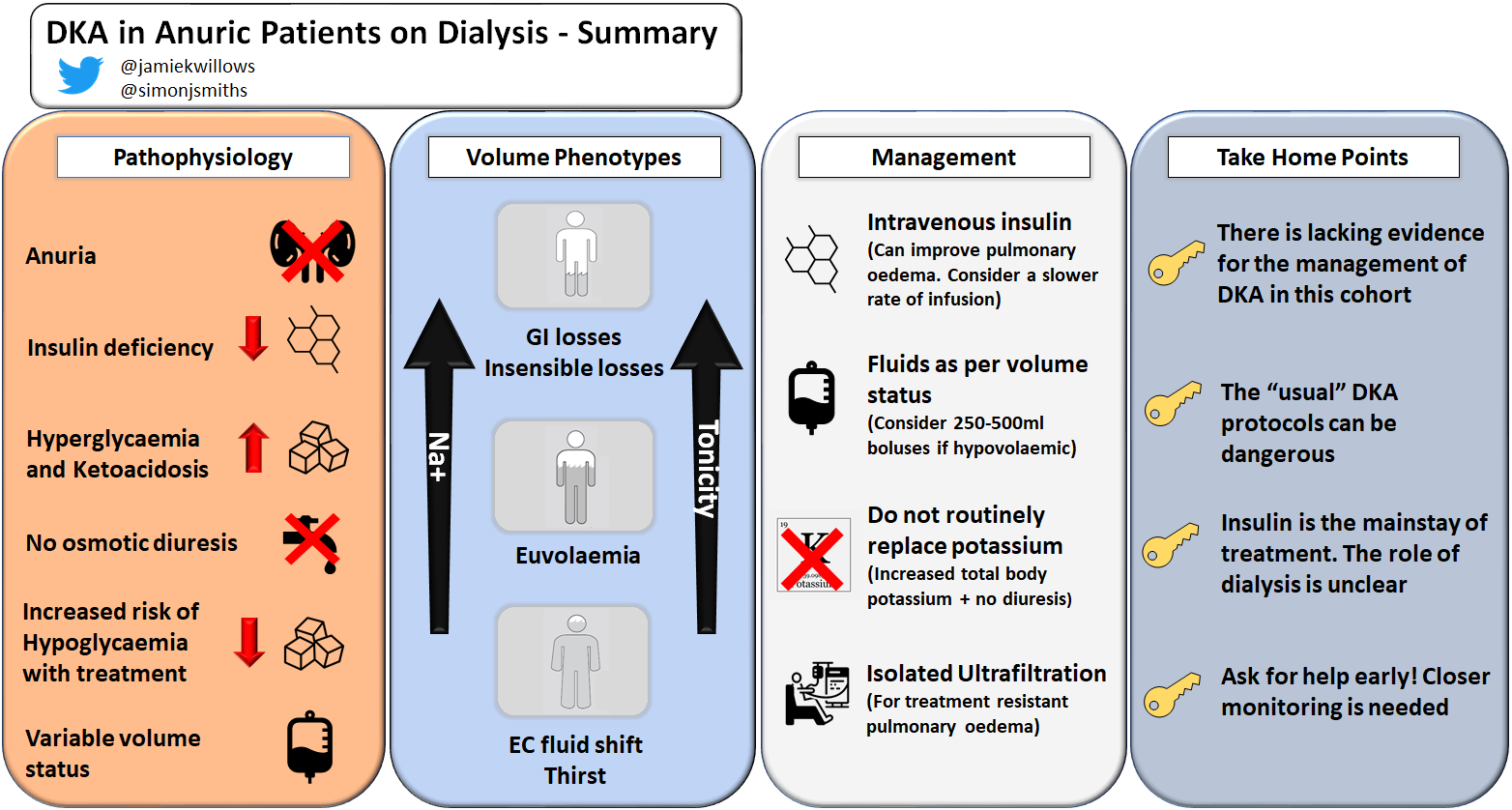
The patient on dialysis with anuria will not get hypovolemic from diuresis or have whole body potassium depletion in the face of hyperglycemia, so when they do develop DKA their pathophysiology (and therefore their management) is distinct. Making the diagnosis can be more challenging given the bicarbonate received during dialysis treatments. In addition, the effects of insulin are long-lasting in the context of kidney failure, and patients on dialysis are more likely to become hypoglycemic during DKA management. Following the usual protocols will therefore result in a life-threatening state of volume overload, hypoglycemia and hyperkalemia – these are patients who need individualized medicine, not the cookbook guidelines.
When it comes to managing DKA in the patients with anuria, it is worth bearing in mind that evidence for recommendations is at the level of case series and expert opinion.
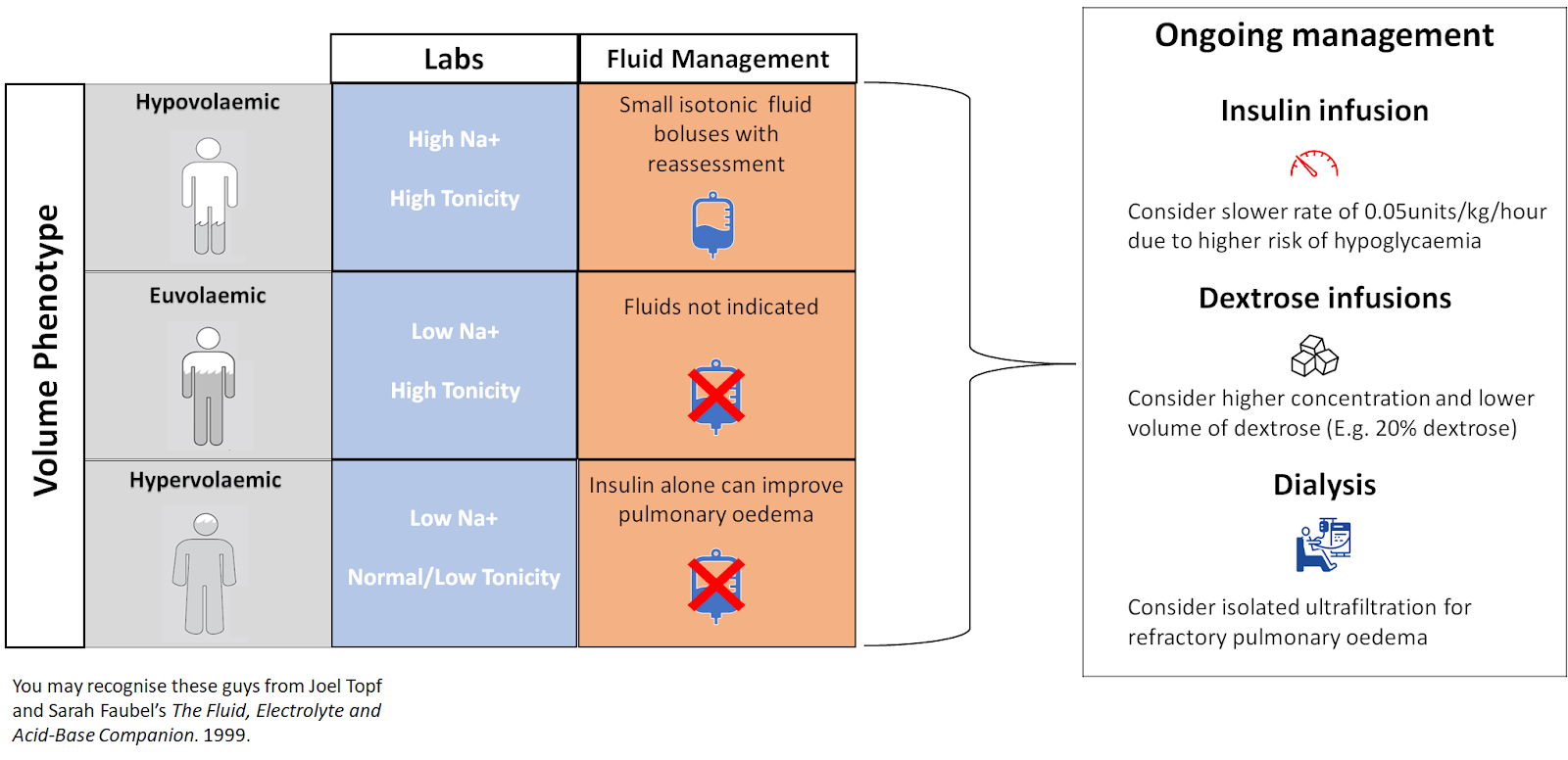
Close attention should be paid to the fluid status. Asking about any preserved urine output is key in the history as those with residual kidney function are more likely to get volume depleted, while recognising that the heterogeneity within this group is also significant – a patient who usually makes one litre of urine per day is very different to the patient who makes 200ml per day in this scenario. Tzamaloukas 2008 described the 3 possible phenotypes of the patient on hemodialysis with true anuria and hyperglycemia.
- Hypovolemic – Although there is no osmotic diuresis, if the history is of days of vomiting, decreased oral intake, or fevers, then the anuric patient may still need volume repletion. The serum sodium and tonicity can be high due to extra-renal water losses. Small boluses of fluid with close monitoring may be necessary, though keep in mind that the need for intravenous medications (or, later, dextrose infusions) will also help get the patient towards euvolemia over time.
- Euvolemic – Serum sodium more likely to be normal, with hyperglycemia contributing to a moderately raised serum tonicity. Intravenous fluids are not indicated initially. If dextrose-containing fluid is required while the ketosis is resolving with intravenous insulin treatment, consideration can be given to using higher concentrations of dextrose solutions to limit the volume inputs.
- Hypervolemic – can occur for three reasons:
i) Hyperglycemia causes extracellular compartment expansion as water is pulled from the intracellular space
ii) The tonicity of the serum glucose causes profound thirst, which can lead to drastically increased oral intake (given thirst is usually considered suggestive of hypovolaemia, it is worth noting that this history finding is unhelpful in this exceptional setting)
iii) Volume overload at baseline / missed dialysis sessions, etc.
The compound result is fluid overload, with low serum sodium and low or normal tonicity. Pulmonary edema and hypertension may be present.
Intravenous insulin replacement is the cornerstone of therapy in all phenotypes. In the hypervolemic phenotype, intravenous insulin therapy may decrease extracellular glucose levels enough to allow water to move back intracellularly – meaning that insulin alone can help improve pulmonary edema!
The rate of insulin infusion is complicated by competing factors of reduced elimination of insulin in patients on dialysis, versus the fact that uremic patients are often more insulin resistant (whether due to hyperparathyroidism, inflammation, metabolic acidosis, or build up of nitrogenous waste). Some expert commentators recommend a slower rate of insulin infusion, and the risks of a more protracted resolution of ketosis should be weighed against the decreased risk of hypoglycemia with this approach. When serum glucose levels fall and insulin-dextrose infusion is required, using higher concentrations of dextrose solutions can be beneficial to limit fluid volume inputs.
Patients with kidney failure and anuria usually have a higher initial serum potassium, and this also often responds to intravenous insulin alone. Increased total body potassium stores (as opposed to whole body depletion in patients with intact kidney function) means that monitoring, but not routine replacement, is warranted. As would be expected, evidence for patients on peritoneal dialysis is even more limited, though some specifically comment that PD can be continued as long as serum glucose and potassium levels are frequently monitored.
But if I have a hyperkalemic, hypervolemic, acidotic patient on maintenance dialysis – why isn’t STAT hemodialysis just the answer?
Well, it might possibly be, but there is no good evidence regarding the harms of hemodialysis in this context – large and rapid reductions in serum tonicity would certainly risk cerebral edema in patients with high serum tonicity. If pulmonary edema or extreme hyperkalaemia are present then dialysis may be emergently indicated. It makes sense to do hemodialysis for as short a time as possible, to limit swings while controlling a specific problem like hyperkalemia, and then go back to usual supportive treatment and close monitoring, even if this approach means the patient needs another short session later the same day. If the indication for extracorporeal therapy is lone pulmonary edema then isolated ultrafiltration could be used, as this will remove iso-osmolar fluid and avoid a tonicity swing.
After hemodialysis the numbers will look fixed, but remember the underlying pathophysiology of insulin deficiency will remain, so make sure insulin therapy is continued. Patients will be more at risk of hypoglycemia during and immediately after dialysis, so should have the rate of insulin therapy reviewed prior to the session. In addition, be mindful that the rapid decrease in serum glucose with hemodialysis will allow water to move intracellularly, so the patient will need to be assessed for intravascular volume depletion after dialysis even if fluid was not removed.
Conclusion
Thankfully DKA is uncommon in patients with kidney failure and anuria . They are protected from insulin deficiency by reduced kidney insulin clearance and, in the case of patients on in-centre hemodialysis, have frequent contact with healthcare professionals to help pick up problems early. However, many patients on dialysis are at high risk of infective and ischemic insults which can trigger DKA, so we need to know the pitfalls of management when they do present and ensure a thorough work-up for underlying causes. In fact, observational studies show that patients on dialysis who developed DKA are significantly more likely to need mechanical ventilation, develop venous thromboembolism, and have prolonged hospital stays, so we should maintain a very low threshold to involve specialists and intensivists early in these patients care.
Ultimately, the management of DKA in patients on dialysis with anuria is somewhat uncharted ground. The familiar and reflexive DKA protocols used in emergency medicine are dangerous for these patients, and must be avoided. Recommendations for this patient cohort are less tried and tested, but follow logically from an understanding of the fascinating underlying pathophysiology.
Reviewed by Amy Yau, Matthew A Sparks, Elena Cervantes


Ed Rutsky well known professor at U of Alabama used to stress that type one diabetics on dialysis should never fast without iv glucose supplementation because of the danger of hyperkalemia from supressed endogenous insulin, it makes sense but I do not know if there has been any clinical evidence.
Ed Rutsky well known professor at U of Alabama used to stress that type one diabetics on dialysis should never fast without iv glucose supplementation because of the danger of hyperkalemia from supressed endogenous insulin, it makes sense but I do not know if there has been any clinical evidence.
This is too beautiful, best explanation ever 👏🏽👏🏽👏🏽