Raphael Rosen, MD
Fellow, New York Presbyterian / Columbia University Medical Center
@RaphyRosen
One of the major challenges in the care of patients on hemodialysis is the establishment and adjustment of dry weight. Strikingly, among the many quality metrics that are monitored by the Center for Medicare and Medicaid Service (CMS), a dry weight assessment procedure is not among them. Physical examination has been shown to be inadequate for detecting volume overload in patients on hemodialysis.
As the use of Point Of Care Ultrasound (POCUS) has expanded among non-radiologists, lung ultrasound has emerged as a promising tool in the assessment of excess lung water in patients on dialysis. A-lines are horizontal repeating lines in regular intervals and are the predominant finding in normal lungs. B-lines are hyperechoic vertical streaks that start at the pleural line and radiate down the lung field in lungs with increased water content. For more background on lung ultrasound, see this RFN post.
Prior studies have demonstrated that increasing numbers of B-lines, in a dose-dependent manner, is an independent predictor of mortality in patients on dialysis. These investigators proposed that lung ultrasound could aid in establishing and titrating dry weight and would result in superior outcomes than standard dry weight assessment.
While the investigators were running their main trial, they spun off a number of impressive papers that whetted our appetite for the main trial. Here are just a few.
- This CJASN paper demonstrates poor sensitivity of physical exam for volume overload.
- This KI paper demonstrates the effectiveness of lung ultrasound in reducing dry weight and ambulatory blood pressure while reducing incidence of intradialytic hypotension.
- This AJKD paper demonstrates improvement of lung ultrasound-guided dry weight reduction in multiple echo parameters of overload and strain.
Based on the findings of improved blood pressure control and cardiac strain after just a few short weeks of intervention, expectations were high for the potential cardiovascular benefit during longer term follow up.
This brings us to the piece de resistance, the main LUST trial (Lung water by UltraSound guided Treatment in hemodialysis patients).
Study sites: The trial recruited patients at 18 dialysis centers across Europe. The trial was funded by the ERA-EDTA (European Renal Association – European Dialysis and Transplantation Association).
Inclusion criteria: Patients undergoing hemodialysis who were at “high cardiovascular risk”, defined by prior myocardial infarction/acute coronary syndrome, stable angina with confirmed coronary disease by angiography, ECG evidence of ischemia, or New York Heart Association (NYHA) class 3-4 heart failure.
Exclusion criteria: Patients with terminal comorbidities (advanced cancer, liver failure, etc), or patients in whom it was technically unfeasible to obtain a lung ultrasound.
Training: The investigators provided an online training course in lung ultrasound to all participating nephrologists. As an assessment of competency, after completing the online training, these nephrologists were provided with videos of lung ultrasound and asked to grade the number of B-lines. They were shown to have excellent inter-observer agreement and agreement with an international expert in lung ultrasound.
Blinding: The treating nephrologists were not blinded as to allocation arm (as they would be the ones performing the lung ultrasound in the intervention group), however, the patients in both arms were assessed every 6 months with lung and cardiac ultrasonography by a cardiologist who was blinded to treatment arm allocation.
The secret sauce (the intervention): In the intervention arm, lung ultrasound was performed monthly. The protocol for lung ultrasound was that the ultrasound probe was placed in 28 anatomical locations throughout the chest and the total number of B-lines was summed. Based on the total number of B-lines across the chest, the following interventions were performed:
| Finding | Intervention |
| Total number of B-lines: <15 | No change in dry weight. Repeat lung ultrasound in 1 month. |
| Total number of B lines: 15-30 | 0.3 kg dry weight reduction over 1 week. Repeat lung ultrasound in 1 week. |
| Total number of B lines: 30-40 | 0.45 kg dry weight reduction over 1 week. Repeat lung ultrasound in 1 week. |
| Total number of B lines: >40 | 0.6 kg dry weight reduction over 1 week. Repeat lung ultrasound in 1 week. |
Intensification of ultrafiltration (UF) was accomplished by prolonging treatment time rather than increasing UF rate to avoid precipitating intradialytic hypotension.
The control arm had dry weight titrated by standard clinical practice. Lung ultrasound was not performed in these patients to make decisions about dry weight changes but was done at 6 month intervals by a cardiologist blinded to treatment allocation as part of the outcome assessment.
Outcomes
Primary: composite of all-cause death, non-fatal myocardial infarction and decompensated heart failure
Secondary: all cause and cardiovascular hospitalization, change in a variety of echocardiographic parameters, patient quality of life questionnaires
Post hoc: (cue the controversy), the investigators added two additional secondary endpoints. They noted two recent cardiology trials that documented reductions in heart failure hospitalizations with lung ultrasound. Thus, they added secondary outcomes of “recurrent heart failure admissions” and “number of repeated cardiovascular events”.
Results: Based on power calculations, they aimed to recruit 500 patients but due to slow recruitment were only able to enroll 363 participants. The patients were well-randomized in terms of baseline characteristics, though the vast majority were Caucasian.
Did they achieve a between-group difference in B-lines? Definitely.
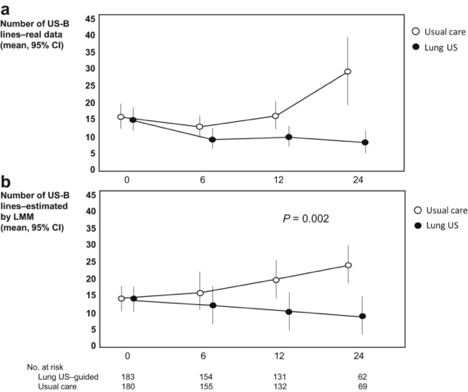
The intervention arm began with a mean of 15 B-lines and at the end of follow up had a reduction in B-lines to 9. The control arm started with 16 B-lines and had an increase in B-lines to 30.
Surprisingly, despite the marked finding of lung decongestion, there was no overall between group difference in the change in dry weight or blood pressure.
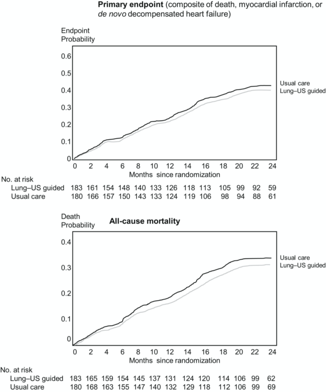
On average, patients had 1.5 years of follow up. The primary endpoint occurred in 34% in the intervention arm vs 39% in the control arm, with a hazard ratio point estimate of 0.88 (95% CI 0.63-1.24) though not significant (P=0.47). None of the pre-specified secondary endpoints achieved significance. However, both post-hoc secondary endpoints favored the lung ultrasound group. There were no increased adverse events in the lung ultrasound group and there was a 1/3 reduction (as seen in a previous trial) in intradialytic hypotension in the intervention arm.
Overall, the trial must be considered a negative trial since it did not significantly reduce the primary outcome. While the point estimate was in favor of the intervention arm, we can only speculate whether under-recruitment led to decreased power to detect the primary outcome. The investigators acknowledge that the post-hoc secondary outcomes, while encouraging, can only be considered hypothesis-generating that lung ultrasound may reduce heart failure admissions. Dr. Carmine Zoccali, the lead investigator of the LUST trial, commented at the recent ASN Kidney Week conference in 2021 that the group will be commencing the LUST 2 trial to specifically study this outcome in a prospective manner.
One final pragmatic comment. While the substudies generated impressive results in dry weight reduction and blood pressure lowering over a short period of time, it is striking that this longer-term trial did not replicate even these findings. It is possible that the lung ultrasound protocol was labor-intensive and, while able to be done rigorously during a brief follow up, it may have proven difficult for the investigators to adhere to this protocol in a more sustained manner. A recent study demonstrated that abbreviated 4-zone lung ultrasound has similar performance in patients on hemodialysis to the well-validated but cumbersome 28-zone protocol.
As lung ultrasound becomes increasingly available, protocols are simplified, and further data is gathered, lung ultrasound is likely to become a valuable tool in a nephrologist’s armamentarium for the assessment of volume status. However, we are still searching for how to best incorporate lung ultrasonography into our practices.
Reviewed by Matthew A. Sparks, MD