A 50 y/o woman presents with symptoms of fatigue and malaise for 1-2 weeks. Medications include ACE, HCTZ, and a multivitamin daily. She had a UTI 6 weeks ago that did not improve after a 5 day course of empiric TMP/SMX and was then given cephalexin for 10 days. Her serum creatinine was 0.7 at the time of her last doctor visit 1 year ago. Now BUN is 35 and creatinine 4.2 and UA has 1+ protein, 3+ blood, and trace leukocyte esterase with specific gravity 1.018 – CBC had no eosinophilia. ANA was 1:40 and complement C3 and C4 were normal. Exam was notable for trace LE edema and no rash.
Urinary sediment showed 10-20 RBC/hpf, all of which were isomorphic. There were no acanthocytes. There were 3-5 WBC/hpf and no bacteria. Scattered tubular epithelial cells were present.
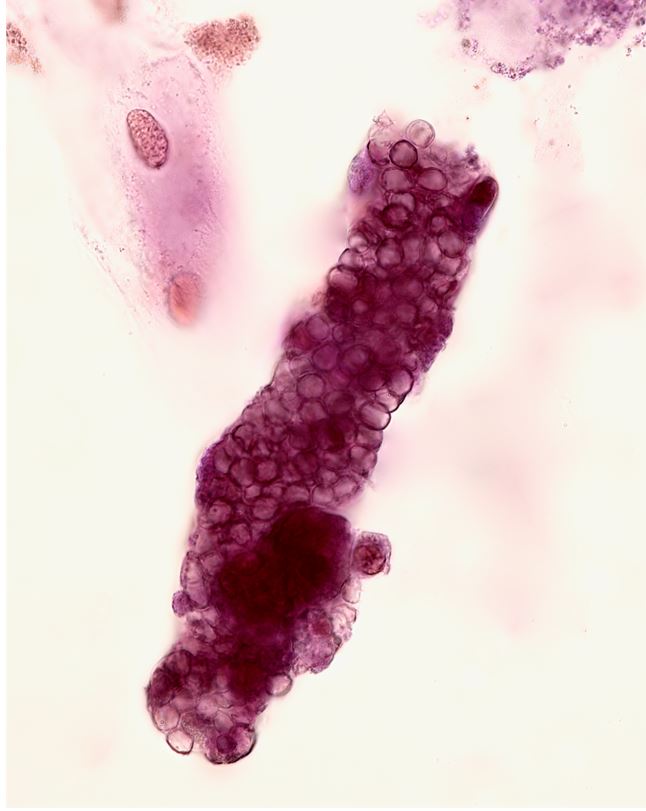
Despite the absence of acanthocytes, there were several RBC casts. There were no WBC casts.

Renal biopsy showed moderate to severe interstitial inflammatory infiltrate (monocytes and eosinophils) and acute tubular injury.
This case is a good reminder that allergic interstitial nephritis does not always present with WBC casts1. Hematuria and pyuria alone may be the most common urinary finding. Remember that red blood cells may enter the tubular lumen via damaged glomerular capillary membranes or damaged tubular basement membranes. In acute interstitial nephritis, intense inflammation may lead to disruption of interstitial vessels allowing extravasation of RBC’s into the tubular lumen via gaps in the tubular basement membrane.
1Fogazzi GB Ferrari B Garigali G Simonini P Consonni D Urinary sediment findings in acute interstitial nephritis. Am J Kidney Dis. 2012; 60: 330–332.https://doi.org/10.1053/j.ajkd.2012.05.002
Post by Jay Seltzer
Edited by Anna Gaddy


I assume that the imaging was normal and urine cultures were negative?
And how does she developed after? The option was for suportive treatment or a course of prednisone?