Maria Angela M. Matabang, MD
Lincoln Medical Center
Acknowledgements: This post is part of a collaboration between The Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. For more information about the ASDIN mission or membership, click here. Special thanks to the ASDIN Education Committee for their support on this project.
Chronic kidney disease (CKD) is an independent risk factor for cardiovascular morbidity. Specifically, among patients with kidney failure, cardiovascular disease (CVD) accounts for 40% of mortality. One of the most common manifestations of CVD in this population is heart failure (HF), which is thought to be influenced by a number of risk factors including age, sex, hypertension, social determinants of health, genetics, volume overload, ischemic heart disease, anemia and hypoalbuminemia. Apart from these an untraditional factor, which is thought to be contributory to HF, is the arteriovenous access.
The gold standard for a safe, long-term dialysis access in patients with kidney failure is an arteriovenous fistula (AVF). Compared to venous catheters, AVFs have considerable advantages in terms of infection risk, access longevity and decreased systemic inflammation. AVF creation is frequently recommended during pre-dialysis care. However, the connection of a low-pressure vein to a high-pressure arterial system is thought to cause vascular remodeling leading to, or exacerbating, heart failure, left ventricular hypertrophy, pulmonary hypertension and heart valve dysfunction.
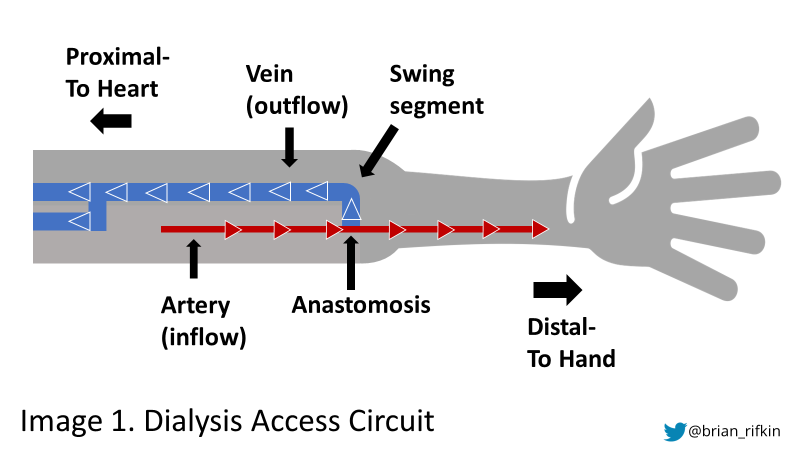
Arteriovenous access creation exposes the patient’s venous system to arterial pressures and flow rates, which cause an increase in wall shear stress (WSS). This signals the endothelium to produce dilating mediators including nitric oxide and endothelium derived hyperpolarizing factor, resulting in venous blood vessel lumen enlargement and subsequent WSS reduction. The production of these mediators, however, may be present for years after access creation.
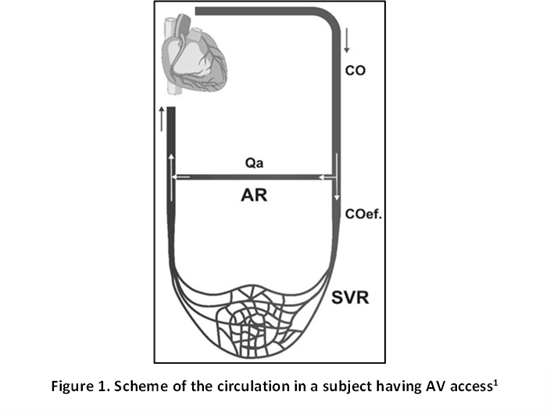
The blood flow of an AV access (Qa), just like any blood vessel is determined by the following relationships:


Qa (access blood flow) is directly proportional to the pressure difference (ΔP) between the peak systolic and diastolic pressures, and the vessel radius (r) to the fourth power. The radius of the blood vessels plays a very significant role in determining Qa. Qa is also indirectly proportional to the access resistance (AR). Thus, a larger anastomosis with a lower AR translates into a higher access Qa.
Figure 1 shows that the AV access bypasses the systemic capillaries, and their associated vascular resistance (SVR), therefore directly contributing to increased cardiac output (CO).
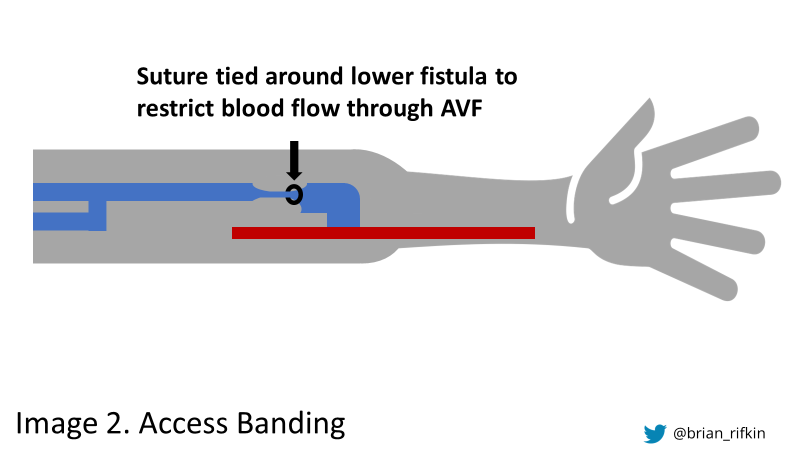
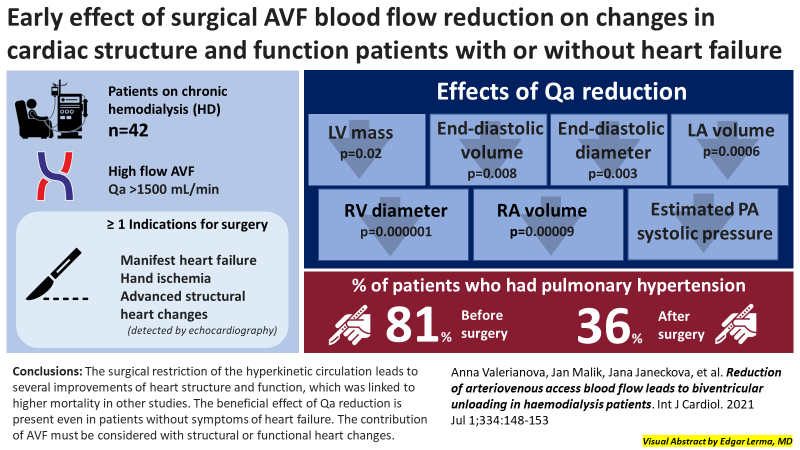
A third order polynomial regression model best defines the relationship between Qa and CO—a curve with an initial CO plateau followed by a steep slope as CO rises more sharply, with greater Qa. It is however important to note that a typical AVF Qa range (0.95-2.21 L/min) is not associated with significantly increased CO. A significant increase in dialysis access Qa does cause “systemic vascular steal”, followed by secondary arterial dilatation with low SVR. A two-center prospective interventional study done by Valerianova et al in 2021 showed that in patients with kidney failure with high-flow AVF (Qa >1500 ml/min) surgical Qa reduction, via banding, caused decrease in left ventricular mass, end-diastolic volume, end-diastolic diameter and left atrial volume. There was also noted a decrease in right ventricular diameter and right atrial volume with a decrease in estimated pulmonary artery systolic pressure.
Two cases of “hyper-acute” high-output heart failure were reported by Bornstein et al. The table below summarizes the demographics, access created and postoperative sequelae. For both patients, at the completion of the procedure, there was noted hemodynamic instability—bradycardia and hypotension for the first patient and hypotension with alteration of mental status for the second patient.
| DEMOGRAPHICS | ACCESS CREATED | SEQUELAE | |
| PATIENT 1 | 40 y/o man with prior echocardiography and catheterization showing pulmonary hypertension with tricuspid regurgitation and 70% stenosis of small, nondominant RCA without ventricular dysfunction | Left leg femoral loop graft with 6-mm x 40-cm Vectra conduit (Bard Peripheral Vascular, Inc, Tempe, Ariz) | Admitted to ICU with initial postoperative echocardiography showing severe pulmonary hypertension with normal ventricular function. With further deterioration; repeat echocardiography showed new right ventricular dysfunction. AV access ligated with repeat echocardiogram showing normalization of right ventricular function. |
PATIENT 2 | 55 y/o woman with cardiac sarcoidosis and severe pulmonary hypertension. Preoperative echocardiography showed moderate to severe tricuspid regurgitation and moderate right ventricular hypokinesis. | Brachial loop graft with 6-mm x 30-cm expanded polytetrafluoroethylene. | Graft clamped during operation with immediate resolution of symptoms. Graft was then briefly unclamped which resulted in recurrence of symptoms. Access was ligated immediately at the operating room.Post operative echocardiography didn’t show changes in heart function. |
In addition, an observational cohort study done by Martinez-Gallardo et al in 2012 showed that 17% (n=95) of CKD stage 4-5 patients who had pre-dialysis AV fistula (AVF) creations developed at least one concomitant episode of acute decompensated HF. After adjusting for known risk factors such as age, female sex, obesity, diabetes and a prior history of HF or CAD, successful creation of AVF still significantly increased HF risk (OR= 9.5, 95% CI: 4.84-18.81, P <0.0001). Among those who had a CHF episode, 47 had functioning AVFs (predominantly upper arm) with a noted median of 51 days from access creation to initial HF episode.
The above mentioned studies and case reports might break a nephrologist’s heart- so how are we supposed to deal with heart failure and AV access creation? The balance between myocardial reserve and AV access flow determines the clinical outcomes of patients undergoing AV access creation. Due to the larger radius of the brachial artery, which is used for creation of upper arm AVFs, there may be a higher risk for high output failure compared with the radial artery for lower arm AVF creation. Hence, the general rule of using the most distal viable access, to preserve venous real estate, may also make sense in preventing HF. Moreover, the cardiac function of the patient with or without HF should be assessed by echocardiogram prior to AVF creation. Consideration of cardiac function should be taken into account when discussing AVF options. The table below summarizes the proposed access selection according to cardiac status in patients with contraindications to peritoneal dialysis.
| Proposed selection of the vascular access type according to the cardiac status in patients with contraindications to peritoneal dialysis (modified from Roca-Tey) | |
| CLINICAL PRESENTATION | TYPE OF VASCULAR ACCESS PROPOSED |
| Life-threatening heart failure | Catheter |
| Left ventricular ejection fraction <30% | Catheter |
| NYHA class IV and ACC/AHA stage D | Catheter |
| Most NYHA class III and ACC/AHA stage C | Catheter |
| ACC/AHA stage A, B and certain C | Distal arm AVF |
| NYHA class I, II and certain III | Distal arm AVF |
Because of the known risk of HF with AVFs, there has been some discussion about whether complete ligation of AVFs should occur at the time of transplantation. Currently, there is still no consensus on AV access management post-transplant, but some studies suggest that AV access ligation may improve cardiac function. A prospective randomized controlled trial by Hetz et al included 28 patients with kidney transplants with 3-24 months of stable graft function (eGFR >30ml/min and eGFR decline <10ml/min during 3-6 months after transplantation), no pre-existing HF and Qa of at least 1500 ml/min. The intervention group had immediate fistula ligation before a 24-month follow up period, while the control group had no surgical intervention. The study revealed that 5 out of 13 (38%) control patients had high-output HF attributable to high-flow fistula compared to none in the intervention group. The authors concluded that prophylactic ligature of the fistula was associated with the avoidance of high-output failure in post transplant patients (p=0.013).
On the other hand, a retrospective exploration of AV access ligation data using United States Renal Data Systems (USRDS) from January 2011 to December 2013 was done showing that out of the 16,845 patients with functioning AVF or graft who received a kidney transplant, only 779 (4.6%) underwent post-transplant AV access ligation. After donor and recipient characteristic adjustments, the following were associated with post-transplant AV access ligation: increasing age, increasing years on dialysis, zero human leukocyte antigen mismatch and steal syndrome. Black race and CHF contrastingly were negatively associated with ligation. The study also showed that a 3-year allograft failure is seen in 4.9% ± 1.3% of those who underwent ligation vs 9.5% ± 0.5% for those who did not, but this result was not statistically significant. Similarly, AV access ligation did not show a significant association with all-cause mortality.
In summary, AVF creation may worsen HF through endothelial mediators stimulated by increased flow and wall stress. Smaller, low flow fistulas may be better for patients with pre-existing HF. Ligation of AVFs may also be reasonable in patients with stable kidney transplant function, but more studies are needed before this becomes a standard of care.
Reviewed by Matthew A. Sparks, Brian Rifkin

Interesting post – thank you for the discussion and work. This is a common conundrum that will continue to be a challenge for nephrology. One additional consideration to add might be the risk of bacteremia and sepsis with a TDC. If someone’s heart is too bad for a AVF placement how are they going to do with Staph in their blood? Pushing forward with PD on patients who have significant CV risk may be ideal if the resources can be put in place.