Welcome to the 28th case of the Skeleton Key Group, a team of 50-odd nephrology fellows who work together to build a monthly education package for the Renal Fellow Network. These are actual cases (without patient identifying information) that intrigued the treating physician.
Written by: Api Chewcharat
Visual Abstract by: Sacha Moore, Bilal Sheik
Tweetorial: Susan Thanabalasigam
A. The Stem
A 45-year-old woman with ductal carcinoma of the breast presented to the emergency room with worsening abdominal pain and shortness of breath. Two months prior, she discovered a breast lump and following a breast biopsy she was diagnosed with ductal carcinoma. Staging CT scans of the chest, abdomen, and pelvis showed metastasis to the liver. She underwent treatment with bilateral mastectomy and chemotherapy with ribociclib and letrozole, which was switched to capecitabine and letrozole after subsequent progression of disease. Two weeks prior to presentation, she was hypercalcemic at 11.5 mg/dL with a normal phosphorus of 2.8 mg/dL. She received 4 mg of zoledronic acid. On presentation, she has worsening shortness of breath and abdominal discomfort. She reports good appetite, and denies fever, dysuria, hematuria, or diarrhea. The nephrology service was consulted for abnormal laboratory values.
Physical examination:
Temperature: 36.7 °C (98 °F) [36.6 °C (97.8 °F)–37 °C (98.6 °F)] Heart Rate: 116 bpm [104–116 bpm]
Respiratory Rate: 26/minute [16–26/minute]
BP: 116/73 mm Hg (116–132)/(57–73)
Oxygen Saturation: 94-96% on room air
General appearance: alert and oriented to time, place, and person, tachypneic
Heart: normal rate and regular rhythm, normal S1 and S2, no murmur
Lungs: clear to auscultation bilaterally
Abdomen: bowel sounds present diffusely, soft and nontender
Extremities: 1+ peripheral edema
B. The Labs
Blood chemistries:
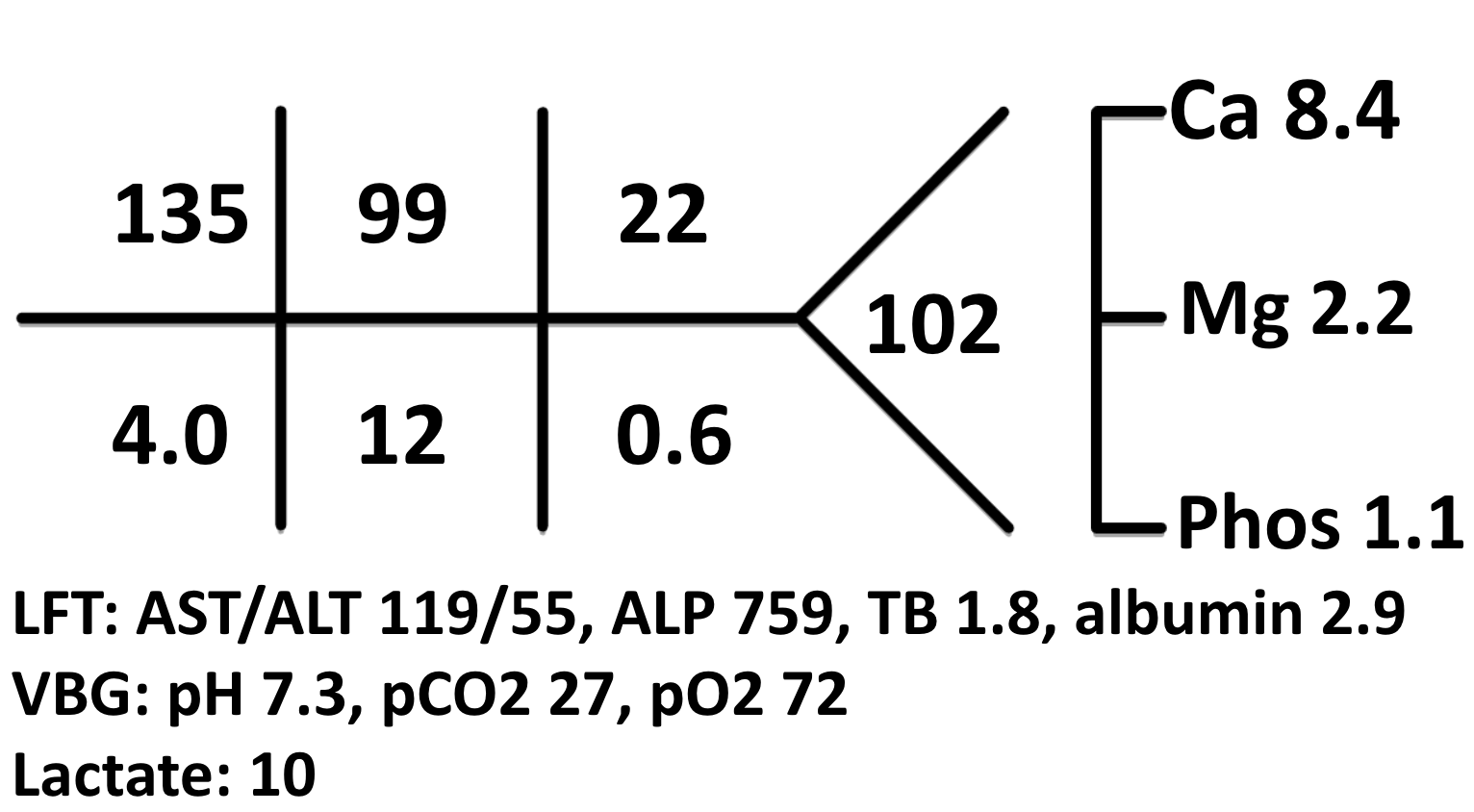
Initial labs in the ED showed
C. Imaging:
CT chest, abdomen, and pelvis done on presentation to the ER showed no pulmonary embolism, but worsening metastatic disease with new lesions in the bone, liver, and peritoneum
C. Differential Diagnosis
- With regards to acid-base disorders, the first step should be to perform an arterial or venous blood gas (ABG/VBG), to confirm metabolic acidosis.
ABG
| pH | 7.30 |
| pCO2 | 27 mmHg |
| pO2 | 72 mmHg on RA |
| HCO3 | 12 mmol/L |
We look back at this infographic to guide us on the steps to interpreting an ABG:
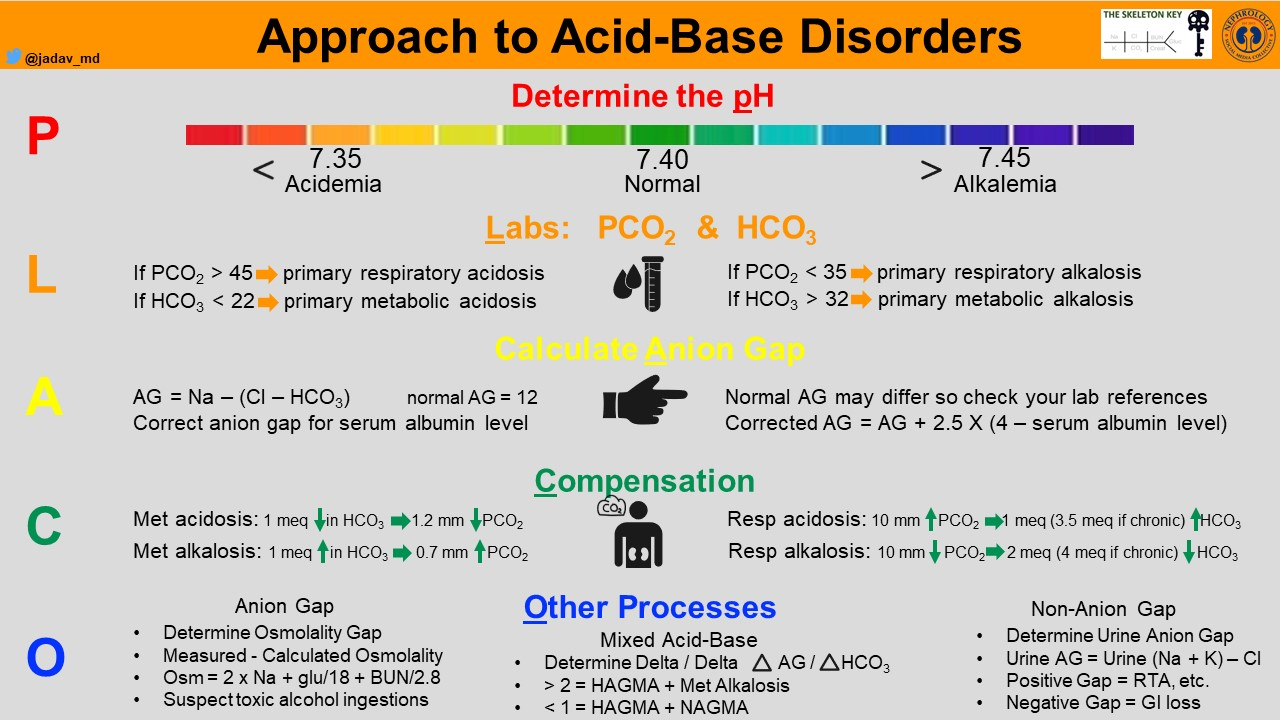
- In her case, the ABG shows high anion gap metabolic acidosis with respiratory compensation
- P (pH): pH of 7.3 indicates an acidemia
- L (labs): CO2 of 12 mEq/L (low) and pCO2 of 27 mm Hg (low) indicates a metabolic acidosis
- A (anion gap): 135 – (99 + 12) = 24 indicates a high anion gap (remember, the corrected anion gap with albumin of 2.9 is 26.8)
- C (compensation): using Winter’s formula, (1.5 x 12) + 8 ± 2 = 24 to 28; our patient’s pCO2 of 27 mm Hg indicates appropriate respiratory compensation
- O (other): delta gap/delta bicarb was 1.25 indicating pure high anion gap metabolic acidosis
How can this acid-base disorder be explained?
High anion gap metabolic acidosis.
The differential diagnosis is presented by the GOLDMARK mnemonic below.

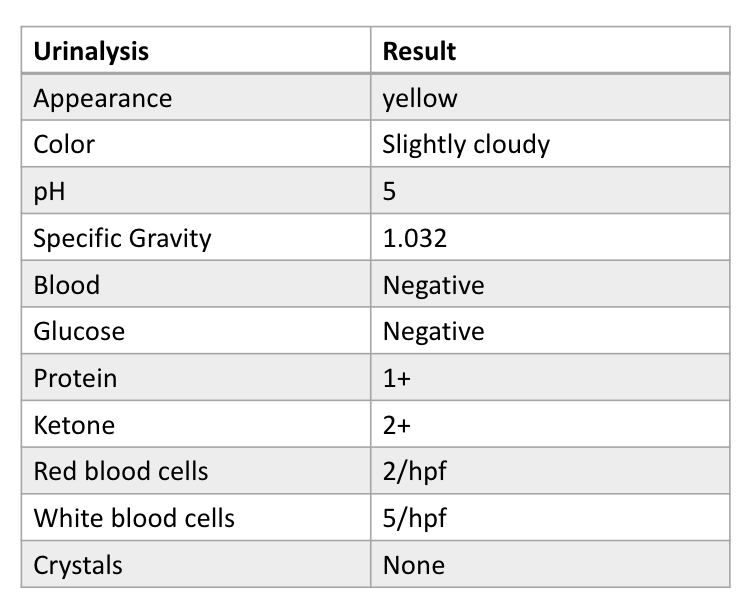
The patient does not report acetaminophen (oxoproline) or aspirin use. There is no history of alcohol use. There were no indications of ethylene glycol or methanol toxicity. There is no history of short gut or abdominal surgery to suggest an elevated D-Lactate. Serum lactate was elevated at 10 mmol/L. Urine was positive for ketones.Therefore, her high anion gap metabolic acidosis is most likely due to lactic acidosis. Also on the differential diagnosis is starvation ketoacidosis; however, her robust appetite pointed against starvation as a true cause. For a deeper understanding of acid base physiology, refer to case #18.
Why does she have lactic acidosis?
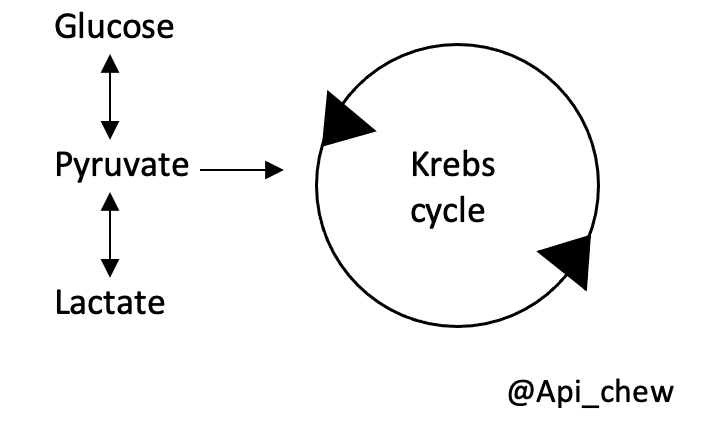
Let’s review the concept of lactic acidosis deeper in this case. Generally, lactic acidosis is defined as serum lactate concentration above 4 mmol/L. Lactic acidosis occurs when lactic production is more than lactic clearance. Lactate is a byproduct of glycolysis catalyzed by lactate dehydrogenase from pyruvate.
There are 3 types of lactic acidosis:
1. Type A lactic acidosis is associated with impaired tissue oxygenation (poor perfusion, cellular hypoxia, or increased metabolic)..
2. Type B lactic acidosis occurs in patients without overt systemic hypoperfusion. Lactic acid is produced by the body when glucose is converted to pyruvate, and then pyruvate is converted to lactate. At the same time, pyruvate can move either though the Krebs cycle or convert back to glucose through gluconeogenesis. Hence, according to the law of equilibrium, processes that increase pyruvate production, prevent pyruvate conversion back to glucose, or prevent pyruvate entry into the Krebs cycle can lead to elevated lactate. (Think about B stands for Biochemistry😂)
What are these processes?
3. D-lactic acidosis occurs in patients with short bowel syndrome, small bowel resection and jejunoileal bypass. Excessive glucose and starch are metabolized by the gram positive anaerobes in the colon leading to production of D-lactic acid. Standard
assay for lactate uses L-lactate dehydrogenase and will not be able to detect D-lactate.
- Her phosphate was low at 1.1 mg/dL with normal corrected calcium of 9.3 mg/dL, normal 25(OH) vitamin D of 24 ng/ml, and elevated Fractional Excretion of Phosphate >20 % suggesting kidney phosphate losses. The hypophosphatemia in this case may have been due to zoledronic acid. There were no other medications associated with hypophosphatemia such as diuretics, valproic acid, insulin, or anticancer agents. Zoledronic acid may induce hypophosphatemia from an increase in parathyroid hormone. Unfortunately, in her case, we did not measure PTH level. Another potential mechanism is Fanconi syndrome from proximal tubule dysfunction. Although our patient did not have glucosuria, it was possible that she might have incomplete Fanconi syndrome. DDx includes FGF-23 tumor-induced osteomalacia. For a closer look at disorders of phosphate homeostasis, please refer to cases #9, 10 and 13
D. Diagnosis
- In her case, lactate was elevated at 10 mEq/L
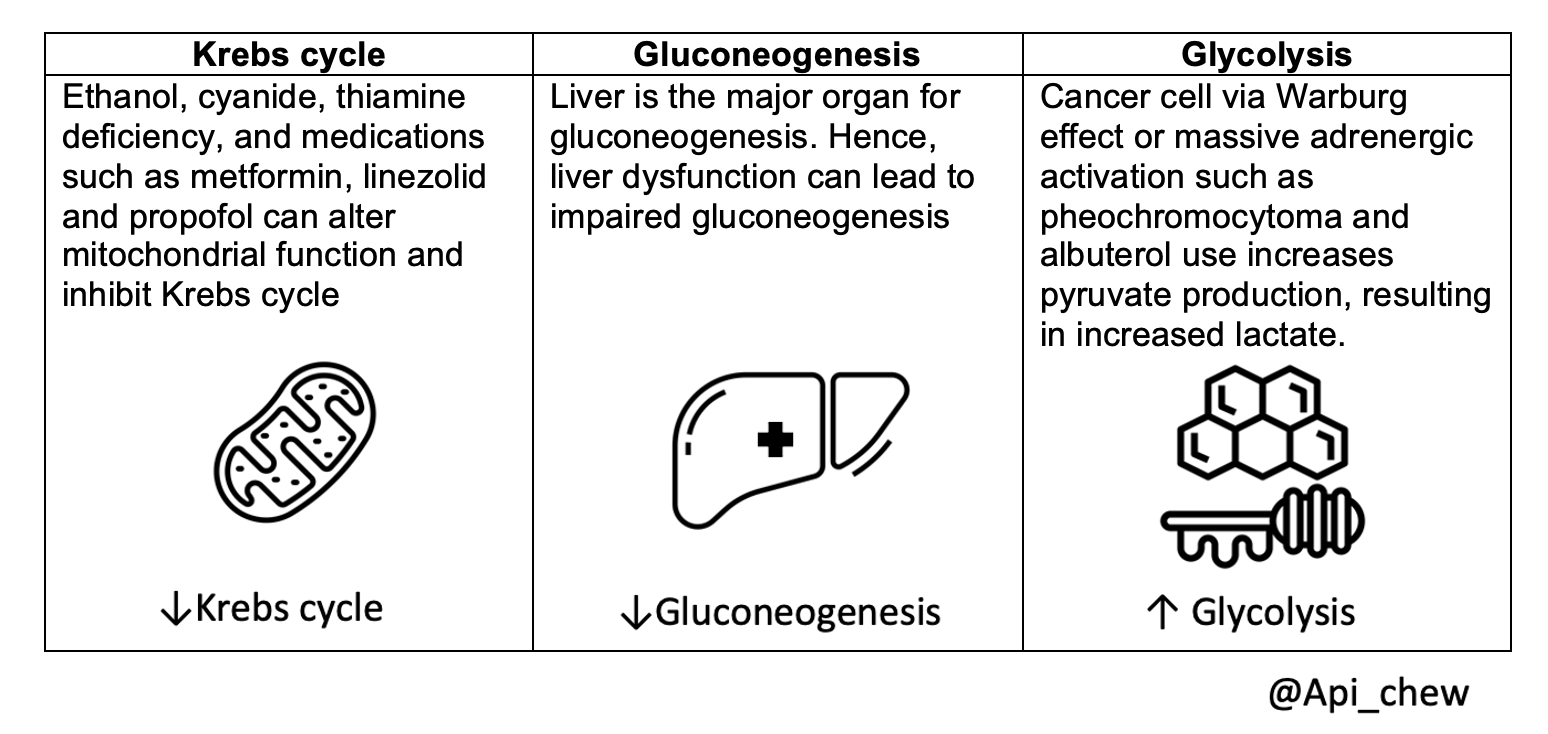
- There was no evidence of hypoperfusion to suggest a Type A lactic acidosis, and thus we consider other causes of a Type B lactic acidosis, either ↓Krebs cycle, ↓Gluconeogenesis, or ↑Glycolysis
- Given there was no medication or toxin present that would affect the Krebs cycle, and no evidence of impaired gluconeogenesis, we are left with increased glycolysis as a possible cause of Type B lactic acidosis
- In this patient with a high burden of metastatic breast cancer, the most likely diagnosis is the Warburg effect
- The Warburg effect happens when tumor cells take up glucose and convert it to lactate even when there is sufficient oxygen to convert glucose to CO2. Although this pathway provides less energy for the cells, high rates of lactate secretion are required to support malignant cell proliferation. The reason is still not fully understood.
- Management of the Warburg effect is limited. Kidney replacement therapy has no effect on lactate level as the rate of lactate production is much more than rate of lactate clearance. Although evidence is limited, thiamine supplementation may ameliorate the Warburg effect by improving mitochondrial function and the aerobic glycosylation pathway
E. Take-Home Points
- Lactic acidosis includes L-lactic acidosis and D-lactic acidosis. L-lactic acidosis includes type A and type B lactic acidosis.
- Type A lactic acidosis is associated with impaired tissue oxygenation
- Type B lactic acidosis occurs in patients without overt systemic hypoperfusion either from 1. ↓Krebs cycle, 2. ↓Gluconeogenesis, 3. ↑Glycolysis
- The Warburg Effect is a Type B lactic acidosis that should be suspected in patients with a significant tumor burden
- The Warburg effect occurs when tumor cells take up glucose and convert it to lactate even when there is sufficient oxygen to convert glucose to CO2
- There is no definite treatment for the Warburg effect. Thiamine supplementation is recommended for the potential benefit for mitochondrial function and poses minimal risk. Thiamine cofactor many enzymes in Krebs cycle and thiamine deficiency known to cause lactic acidosis
Reviewed by: Matthew A. Sparks, Margaret Deoliveira, Joel Topf, Jefferson L. Triozzi, Raad B. Chowdhury, Isabelle Dominique Tomacruz, Sai Santhoshini Achi


Not the biggest problem above, but an ionized calcium (iCa) measurement could be useful here. In spite of the normal “corrected calcium” noted in the text above, as well as the acidemia, it is probable that moderate ionized hypocalcemia is present, as a result of chelation by lactate, with the true iCa value likely between .98 mM and 1.21 mM, suggested by using this calculator:
https://qxmd.com/calculate/calculator_704/predicting-ionized-hypocalcemia-in-critical-care