Sherida Edding MD, IM PGY-3 Lincoln Medical and Mental Health Center
Andrew Kowalski MD, MPH, FASN, Nephrology Associates of Northern Illinois, Loyola University Stritch School of Medicine/ Macneal Hospital
Acknowledgements: This post is part of a collaboration between The Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. For more information about the ASDIN mission or membership, click here. Special thanks to the ASDIN Education Committee for their support on this project.
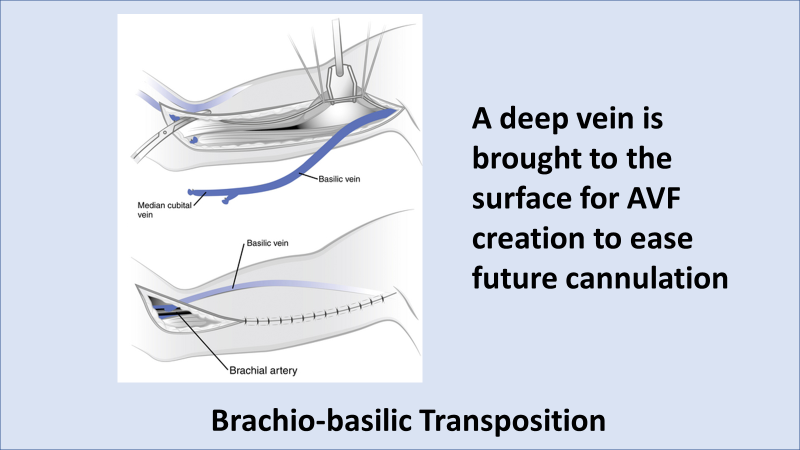
The National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) and the Fistula First Initiative recommended that arteriovenous fistulas (AVFs) should be considered as the preferred initial conduit for hemodialysis in patients with kidney failure, followed by arteriovenous grafts (AVG) and finally central venous catheters (CVCs). Even though Fistula First has been replaced by the ESKD Life Plan (the right access, in the right patient, at the right time) AVFs remain the AV access of choice for a majority of patients. An AVF is a surgically created conduit where an artery is anastomosed to an adjacent vein. The most common AVF sites include the radiocephalic fistula, brachiocephalic fistula, and transposed brachiobasilic fistula (Figure 1).

AVFs are proven to have superior clinical and economic advantages compared to other forms of vascular access. AVFs have longer primary patency rates (average of 3-5 years) and significantly decreased rates of complications including infection, access dysfunction, central venous stenosis and mortality. However, the benefits over CVCs are only appreciated once the access has actually matured and is usable for dialysis therapy.
AVF maturation is a dynamic structural and functional remodeling process facilitated by the release of nitrous oxide and the breakdown of elastin to permit dilatation of the outflow vein, leading to a dramatically increased blood flow. For example, mean blood flow in the radial artery can increase ten-fold once an AVF is successfully mature. In a similar manner, mean blood flow in the brachial artery, about 220 ml/min at baseline, often increases to over 1000 ml/min in a mature fistula. In a comparable way, the veins utilized for dialysis access develop enlarging diameters, with a thickened muscular layer, thereby creating a suitable area for repeated needle puncture (so called “fistula cannulation”).
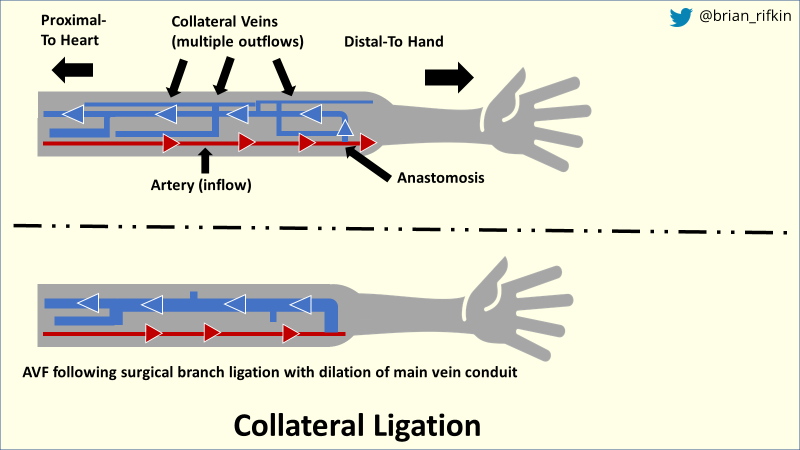
There is no universal definition for clinical AVF maturation. However, the “rule of sixes” proposed by the KDOQI guidelines has been widely used, though not validated. Six weeks after creation a mature AVF should achieve a blood flow of at least 600 mL/min, a diameter of at least 6 mm, a 6 cm area suitable for cannulation, and a depth of 6 mm or less from the skin surface. Unfortunately, a substantial proportion (30%–60%) of AVFs fail to mature adequately due to early thrombosis, anastomotic stenosis, lack of vein and artery dilation due to intimal hyperplasia, vein scarring, large diverting accessory veins, veins too deep to cannulate and other factors. Some of these issues can be corrected by early interventions like angioplasty, transposition (surgically raising deep veins to the surface) or collateral ligation as seen in Figure 2.
AVF maturation failure is described as a fistula that is never usable for dialysis or that fails within three months of initial use. Patients with high-risk of AV access failure include those who are elderly or female due to smaller vascular anatomy. In addition, patients who have a history of CVCs or peripherally inserted central catheter lines (PICC lines), cardiac pacemakers or other devices may have damaged or stenotic central and peripheral blood vessels (Fig. 3). Finally, comorbidities such as peripheral vascular disease and heart failure may lead to primary AVF failure. Poor vasculature makes for difficult targets for anastomosis creation. Also, as discussed in our last ASDIN RFN blog, AV access creation can lead to worsening heart failure symptoms occasionally requiring access banding or even ligation.
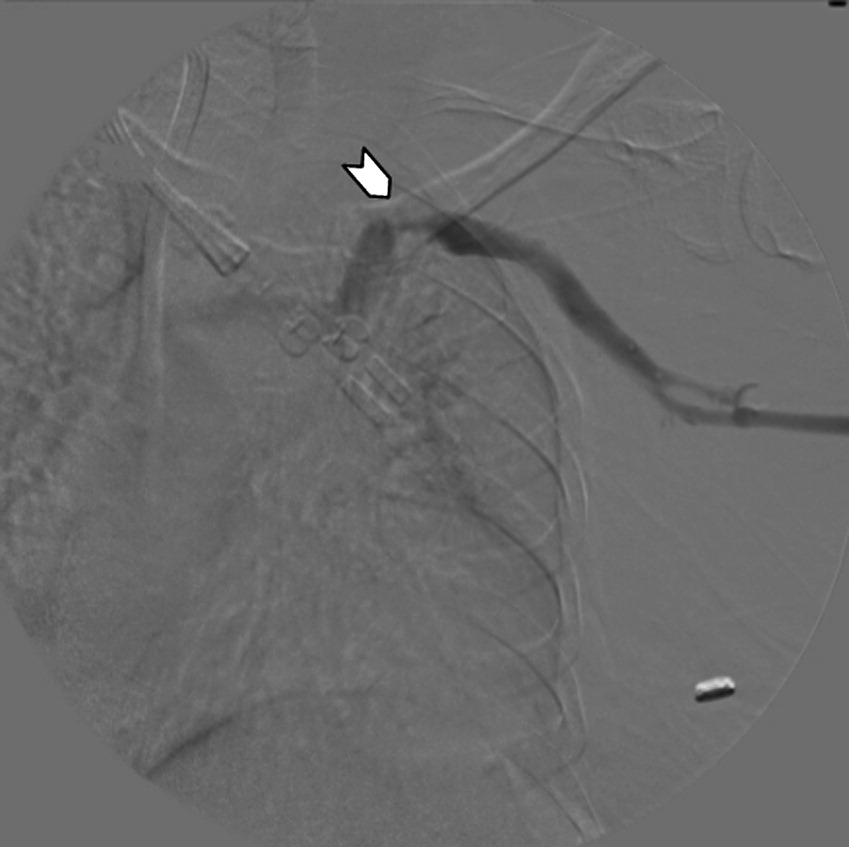
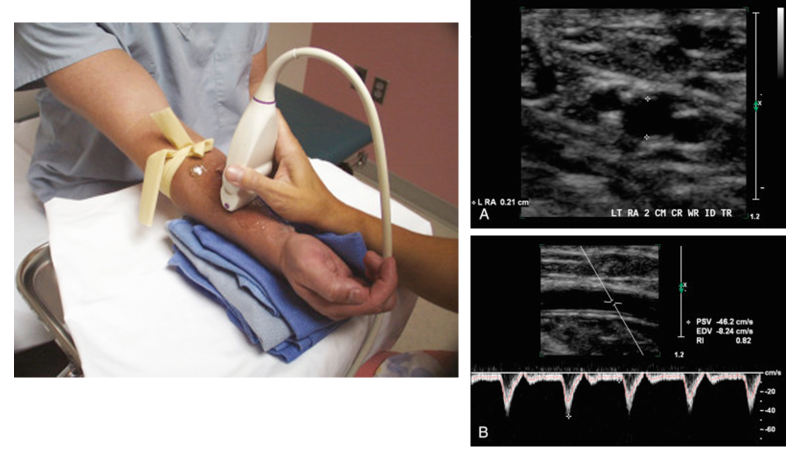
Vessel anatomy and its remodeling are required for successful maturation of an AVF. Preoperative evaluation of the vessels using duplex ultrasound and/or a venogram for “vein mapping” is often done to assess the structural and functional aspects of arteries and veins (Fig. 3). Furthermore, in patients who are high-risk for AV access failure, it confers an added benefit of being able to determine the correct choice of initial AV access location. To optimize successful creation, the KDOQI guidelines suggest having a vein diameter of 2.0 mm to 2.5 mm, an access segment of 6 cm for cannulation, and patent central and draining veins. In conjunction with KDOQI, The Society of Vascular Surgery (SVS) recommends placing access as distal in the upper extremity as possible to preserve future central access while giving preference to the non-dominant arm.
Both the KDOQI and SVS guidelines recommend postoperative monitoring and surveillance of an established access, though the level of evidence to support this is low. Current practice maintains an evaluation to be conducted four to six weeks after creation, with subsequent evaluations as needed. Various methods can be used to assess the functionality of AV accesses ranging from clinical physical evaluation to invasive angiography.
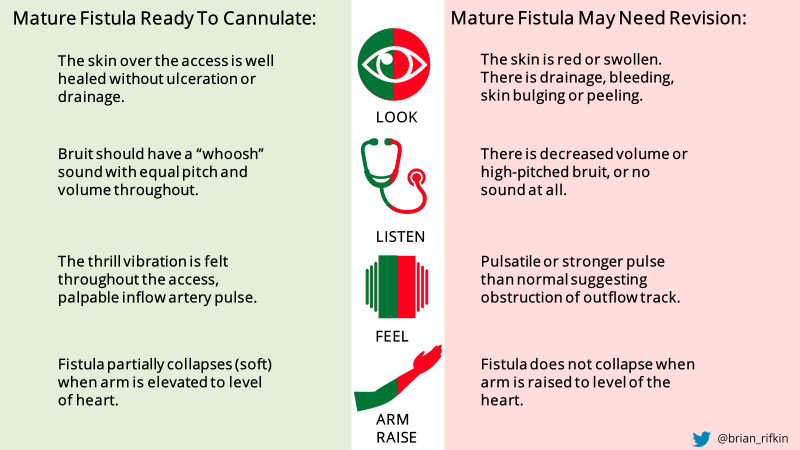
The clinical assessment of a new AVF requires expertise in interpreting visual, auditory, and tactile clues (Fig. 4). Physical examination can be accurately used to determine when an AVF can be cannulated and used for hemodialysis in about 70-80% of patients. Abnormalities on physical examination of the access have a high positive predictive value for stenosis, estimated at nearly 80%. Physical exam is a reproducible, accurate, noninvasive, and inexpensive test in the hands of an experienced observer.
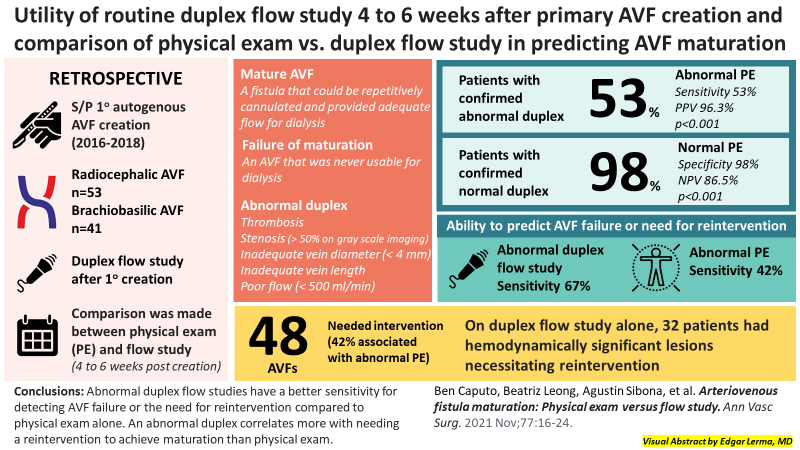
Duplex ultrasound imaging can assess the access for both anatomic and flow abnormalities that may represent significant stenosis – blood flow, vessel diameter, depth of fistula and presence of anatomic lesions. Several small, single-center studies have used postoperative ultrasound to predict AVF clinical maturation. Caputo et al (2021) conducted a single-center retrospective review of 155 veterans with primary AVFs to determine the utility of routine postoperative (4-6 weeks after) duplex ultrasound and compare its predictability of fistula maturation with physical examination alone (Fig 5). Their study revealed that there was a significant association between physical exam and duplex ultrasound studies. Of the patients with a confirmed abnormal duplex ultrasound, 53% had an abnormal PE. Of the patients with a confirmed normal duplex, 98% had a normal PE. Although the presence of an abnormality on physical exam is highly specific for an abnormal duplex (98% specificity), it lacks the sensitivity to identify potentially correctable issues (53% sensitivity). The authors therefore advocated for the routine use of a postoperative duplex flow study to identify potentially correctable issues and optimize fistula maturation.
Patients also have a role in helping their AVF mature by doing upper limb exercise. It is considered part of routine clinical practice, although there are only a few small studies available. In a study by Leaf et al. (N = 5), doing a 6-week ipsilateral isometric hand-grip exercising and repetitive squeezing of a soft ball resulted in an increase in the size of the studied vein. It is hypothesized that exercise increases blood flow that subsequently causes increase in the diameter of the outflow vein. It is advised that these exercises are best done 2 weeks after surgery, once the incision site has healed. Hand exercises are easily accomplished by the patient at home. Patients can be advised to squeeze a ball 10-15 times a minute for 1-2 minutes several times throughout the day. Although it is difficult to draw significant conclusions about the benefits of such practices due to the limited studies, hand exercises are inexpensive and low risk.
In conclusion, there is still a lot to learn about the science of AVF maturation. Further studies are required to understand the underlying mechanisms and predictors of maturation failure. In addition, standardization of postoperative monitoring techniques as well as techniques to promote AVF maturation are needed to improve success rates. In the meantime, careful pre and postoperative measures of flow, diameter, and depth will enhance the probability of success in clinical AVF maturation.
Reviewed by: Brian Rifkin, Margaret DeOliveira, Matthew A. Sparks