Dr. Avinash Rao Ullur, MD,
Clinical Fellow in Nephrology,
University of Toronto, Canada
avinash.raoullur@uhn.ca
Acknowledgements:This post is part of a collaboration between The Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. For more information about the ASDIN mission or membership, click here. Special thanks to the ASDIN Fellows Education Committee for their support on this project.
Introduction: Amongst the various aspects of chronic kidney disease (CKD) management, decisions regarding vascular access creation are critical. A homogeneous approach of opting for arterio-venous fistulas (AVFs) as the solitary best choice, and central venous catheters (CVC) as the worst (based upon observational studies) has marginalized the importance of patient preference. The recent KDOQI 2019 guidelines have put aside the “one-size-fits-all” strategy. KDOQI now advocates for the right access, in the right patient, at the right time, for the right reasons. The end stage kidney disease (ESKD) Life-Plan (Fig. 1), discussed in the KDOQI guidelines, takes into consideration the combined goals of patients and the care team to aid in the transition from CKD to kidney failure. A patient tailored approach in vascular access creation gives patients’ a pathway to negotiate their interests, desires and needs during dialysis access creation and management.
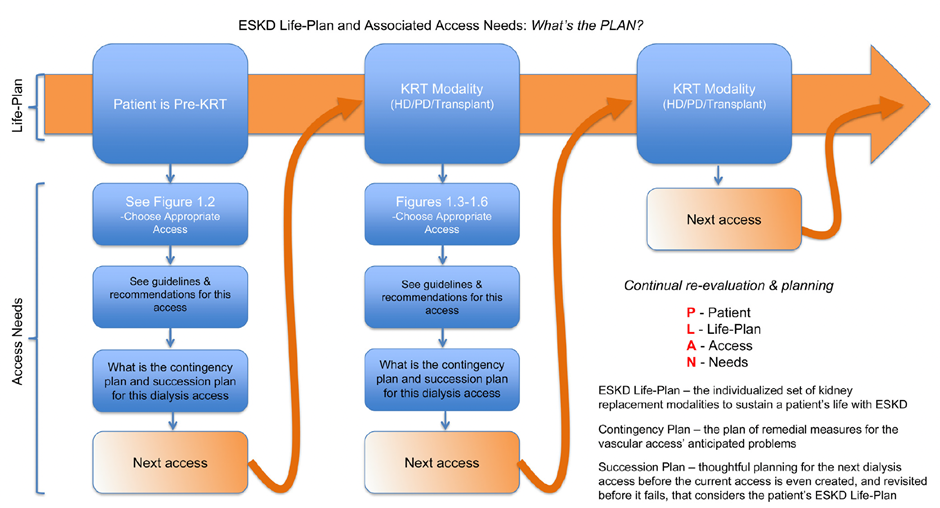
Fig 1. ESKD and Dialysis Access Life Plan – KDOQI 2019
Why is shared decision making needed?
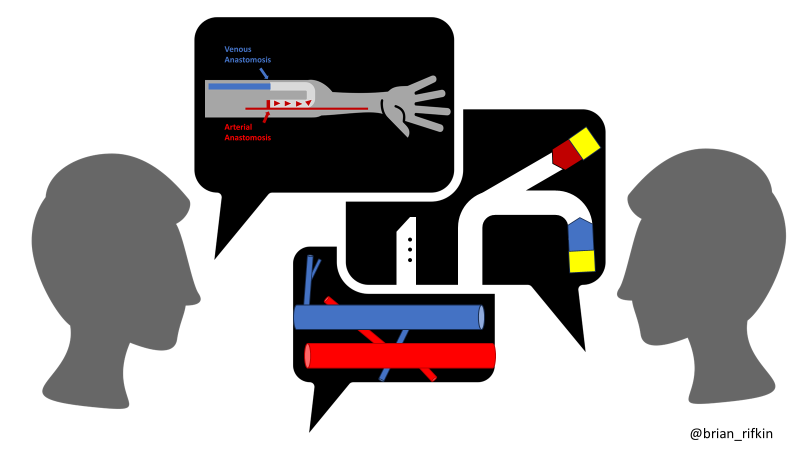
Shared decision making has been defined as an approach where clinicians and patients share the best available evidence and opinions when faced with the task of making medical decisions. Patients are supported to consider options and achieve informed preferences. For patients requiring dialysis, the decision to undertake the creation of various types of vascular accesses including AVFs, arteriovenous grafts (AVGs) or CVCs depends upon individual biological factors, preferences and clinical needs. Emotional factors including needle phobia and worrying about pain or disfigurement also influence patients’ choice of vascular access. Up to 30% of patients eligible for AVF creation decline the procedure. Reasons given included anxiety induced by peer group descriptions and concerns surrounding the vascular access adversely affecting daily activities. Additionally, the choice of vascular access may be influenced by comorbidities, vessel suitability, functional status, and perceived quality of life. Physicians must consider all the clinical complexities surrounding a particular individual, and the patient’s opinion, to strike a balance and achieve shared goals.
Considerations for achieving the right vascular access at the right time for the right patient. Woo K and Lok CE .Clin J Am Soc Nephrol. 2016 Aug 8; 11(8): 1487–1494.
In the paper by Murea et al, four important barriers for shared decision making were identified and discussed.
1. Knowledge gaps: Lack of reliable tools to assess outcomes of AVF creation has been a challenge for physicians discussing access procedures with patients. When compared with other types of access for patients on dialysis, CVCs have the highest association with infections, cardiovascular complications and death. However, patients who initiate dialysis with CVCs tend to have more comorbidities (in comparison to the patients who start with AVF), and thus the outcomes of these patients may not be comparable. Next, lack of discussion regarding the need for AVF revision and secondary access creation after the failure of AVF can perpetuate false notions about the “permanency” of AVFs. Where applicable, a detailed discussion on various types of accesses with their effects on routine life and well-being needs to be brought up to help patients to make rational choices (Table 1). Furthermore, improved availability of knowledgeable physicians or vascular access coordinators might influence patients’ decision making. Additional studies are required to compare the use of various vascular accesses in diverse clinical scenarios.
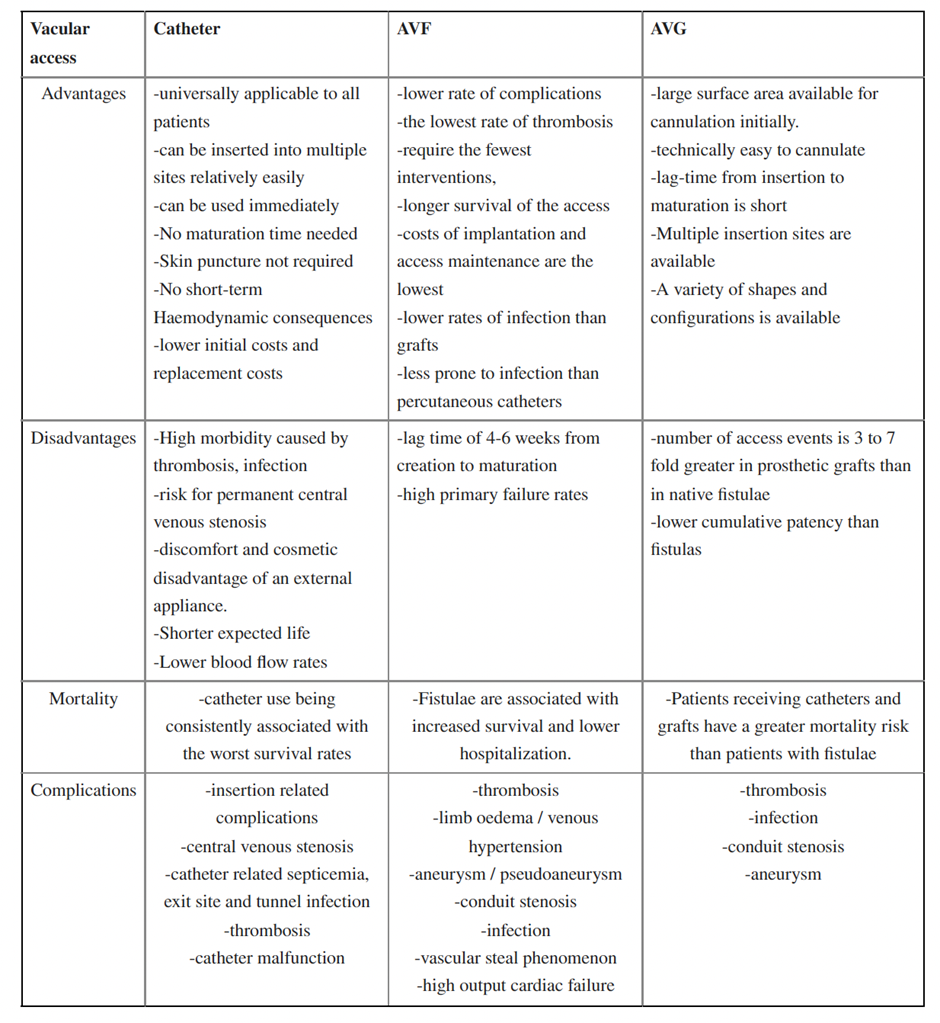
Table 1. Comparison of various types of vascular accesses – Hemachander R. J Clin Diagn Res. 2015 Oct; 9(10): OC01–OC04.
2. Physician factors: Many physicians face limitations when discussing dialysis access. Deliberation can be limited due to lack of patient and physician time. Also, physician fear of not reaching performance indices and inflexible ideology on the type of access required by dialysis administrators may limit discussion. Unfortunately, some physicians or access coordinators may be uncomfortable letting patients choose their vascular accesses, which leads to further shortfalls in communication. Additionally, physicians may not have been trained to discuss the intricacies of dialysis access, which creates hurdles in exposing the patients to available innovations. Unfortunately, and all too common, patients may not know the reason behind why a particular access was chosen. It has been shown in the studies that lack of thorough explanation, coupled with adverse access events, drives patients to switch caregivers. A genuine conversation regarding the vascular access expectations between physicians and patients would potentially alleviate patient dissatisfaction.
3. System based factors: Current policies and systems have attempted to improve patients’ experiences on dialysis. Unfortunately, vascular access compromise does not always align with the quality performance metrics of healthcare administrators. For the widespread advancement of vascular access care and patient experience, incentive structures and pay for performance models need to be modified accordingly. Nephrologists should have the freedom to make decisions about vascular access while taking into consideration patient choice rather than unyielding, system-driven recommendations. Documenting an ESKD Life-Plan for access needs, and tailoring the policies to include patients’ preferences, would be most beneficial in improving the patient’s perceived quality of care.
4. Patient factors: To make an informed decision on the type of vascular access, it is essential that patients know the risks and benefits of AVFs, AVGs and CVCs. Medical literacy regarding method of creation, procedure related complications, adjuvant procedures to aid maturation, timing of use, incidence of infections, access failure rates and alternative options need to be discussed by the physician. The effect of dialysis access on daily activities as well as a patient’s work-life also deserve consideration. Visual aids, electronic education and introductory visits to the dialysis units could help patients make a more informed decision about vascular access creation. Peer-to-peer discussions with patients on dialysis may be especially beneficial given patients on dialysis firsthand experience. Early engagement and timely referral to access creation also influence the patient outcomes.
Age is also an important determinant in planning the type of vascular access. First, CKD progression is typically slower in elderly. Next, the loss of vascular elasticity and increased intima-media thickness could be potential factors affecting the AVF maturation. In fact, older patients have a 37% risk of primary AVF failure as compared to non-elderly individuals. Even among elderly patients who have had AVF created prior to initiation of dialysis, only about 47.7% start dialysis with AVFs due to delayed maturation. Considering all these factors along with life expectancy among older adults plays a crucial role in planning the vascular access.
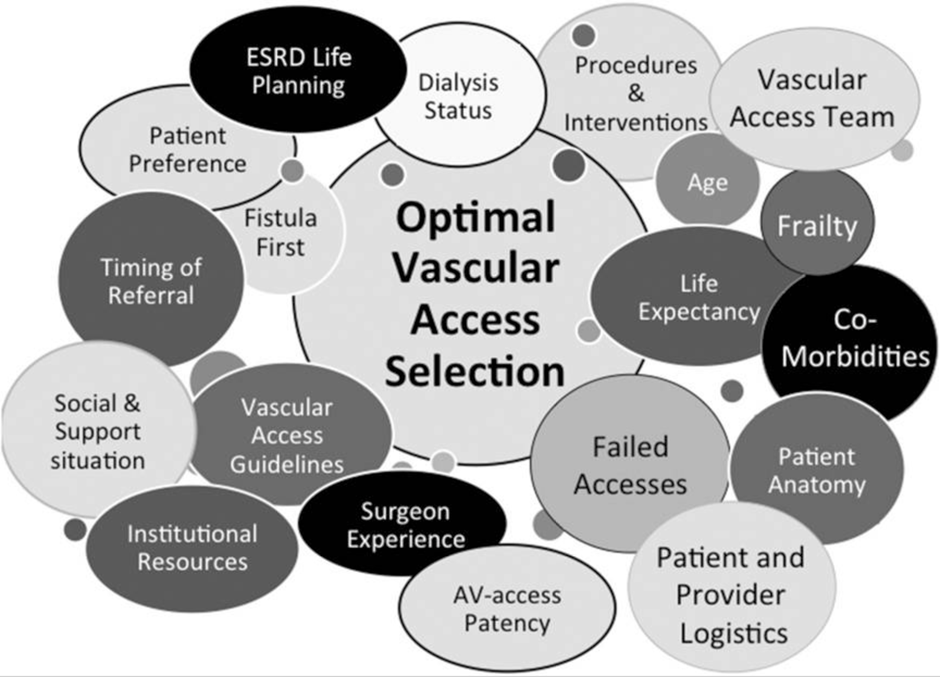
Other important factors to consider during shared decision making: The current standard of vascular access practice is based upon observational evidence derived decades ago and needs reevaluation (Fig 2). There are currently no validated clinical tools to assess the surgical outcomes of vascular access creation to help patients navigate expectations. A systematic review of 46 studies revealed 6 themes which described patients’ perspectives on vascular access initiation and maintenance in dialysis: heightened vulnerability, disfigurement, mechanization of the body, impinging on way of life, self-preservation and ownership, and confronting decisions and consequences.
It is not uncommon that patients seek opinions from family members, relatives and friends who are familiar with a patient’s daily routine. Involving caregivers, along with the patients, during counseling on vascular access may help in integrating complex factors including socioeconomic factors, religion, literacy and cognitive ability. Friends and family may help in translating details in patient friendly language and reiterating information following the visit.
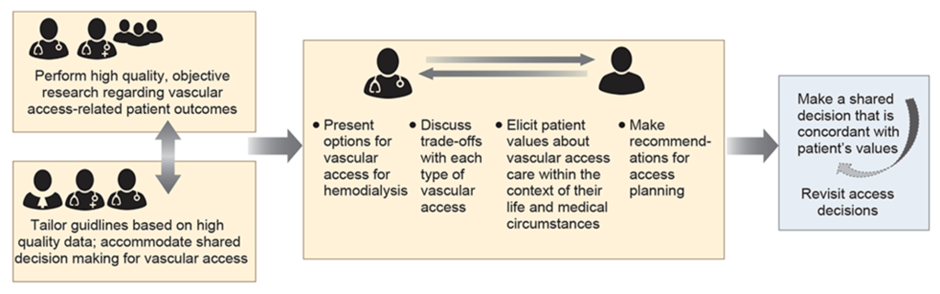
Fig 2. The fundamentals of shared-decision making for hemodialysis vascular access planning and care – Murea et al.Kidney Int. 2021 Oct; 100(4): 799–808.
Conclusion: The principle of “primum non nocere” (first, do no harm) should always be acknowledged in planning a patient’s vascular access. Availability of skilled surgical specialists and well-trained dialysis nurses help in reducing the need for secondary interventions and pain during access cannulation. Physicians need to be willing to negotiate with patients and caregivers to address individual needs. The type of access and potential alternatives need to be given consideration, and physicians should not compel the patient to only one type of access. Future studies should aim at comparing the outcomes of vascular accesses in various dialysis populations, while building tools to answer the prevailing unsettled questions in dialysis access care. Finally, physicians and patients can be hopeful that innovations in vascular access design and engineering might further improve patient acceptance and comfort in the near future.
Reviewed by Matthew A. Sparks, Brian Rifkin, Margaret DeOliveira
