Sandhya Suresh, MD DrNB
@Sandyrvsdav
NSMC 2022
Department of Nephrology, SRIHER, Chennai, India
Introduction: Acute Kidney Injury (AKI) affects nearly 13.3 million people every year with 85% of the cases occurring in the low and middle-income countries. Several epidemiological studies have shown that AKI is associated with higher risk of death, development of chronic kidney disease (CKD) and accelerated progression to kidney failure, with the accompanying burden of high long-term costs as well as poor quality of life. While the standardization of definitions and staging criteria for AKI have led to better epidemiological assessment of the global AKI burden, there is need for greater attention to the outcomes of AKI. Most AKI trials use biomarkers of kidney dysfunction such as creatinine and cystatin C as endpoints. However, these markers serve as surrogate endpoints and are not reflective of ultimate clinical events and are also associated with several limitations. While they may be suitable for phase I and II studies, key patient-centered outcomes should be incorporated as endpoints in phase III clinical effectiveness trials in established AKI. The need for clinically meaningful outcomes as AKI clinical trial endpoints was put forth in the early 2010s in order to improve the understanding of AKI and to determine the effect of different interventions and the link between AKI and persistent morbidity. These hard outcomes would have to be objectively and easily measurable, consistent across different populations and reflective of the effect of AKI on the long-term health of individuals.
Defining MAKE: The NIDDK (National Institute of Diabetes and Digestive and Kidney Diseases) conducted the “Clinical Trials in Acute Kidney Injury: Current Opportunities and Barriers” workshop in 2010 where they put forth that a combination of death, dialysis and sustained loss of kidney function would be appropriate endpoints for phase 3 studies. The term MAKE (Major Adverse Kidney Event), analogous to MACE (Major Adverse Cardiovascular Events) after coronary artery disease, was thus introduced as a consensus composite outcome which includes the following events:
- Death
- new requirement for dialysis
- worsening of kidney function denoted by ≥ 25% decline in the estimated glomerular filtration rate (eGFR) from baseline.
Use of a composite outcome allowed the recording of a greater number of clinically significant events after an AKI episode and could increase the statistical power of studies assessing the efficacy of therapies. MAKE has been reported at different time frames after an AKI in different studies. Some studies also report outcomes as time-to-first-event among the MAKE outcomes while others report absence of MAKE as primary outcome indicating renal-disability free-survival.
Incidence of MAKE after AKI: In most clinically enriched populations with greater severity of AKI, the incidence of MAKE is expected to be approximately 30%. Studies in critically ill populations report short-term MAKE incidence at discharge and at 30, 60 and 90 days as MAKE-DC, MAKE30, MAKE60 and MAKE90 respectively. Major landmark trials analyzing the efficacy of interventions such as the SMART and SALT-ED trials have used MAKE30 as the primary or secondary endpoints. The incidence of MAKE30 in ICU patients has ranged from 16% to 28%. MAKE30 has been reported at a rate of 9.6% after an episode of AKI related to sepsis in the pediatric population. MAKE30 has the advantage that it is easy to measure, affordable and is associated with less loss to follow-up than longer-term MAKE endpoints. MAKE30 is limited by the concern that the early mortality may not be attributable to AKI itself. However, this endpoint is related to persistent kidney dysfunction and is therefore a meaningful endpoint.
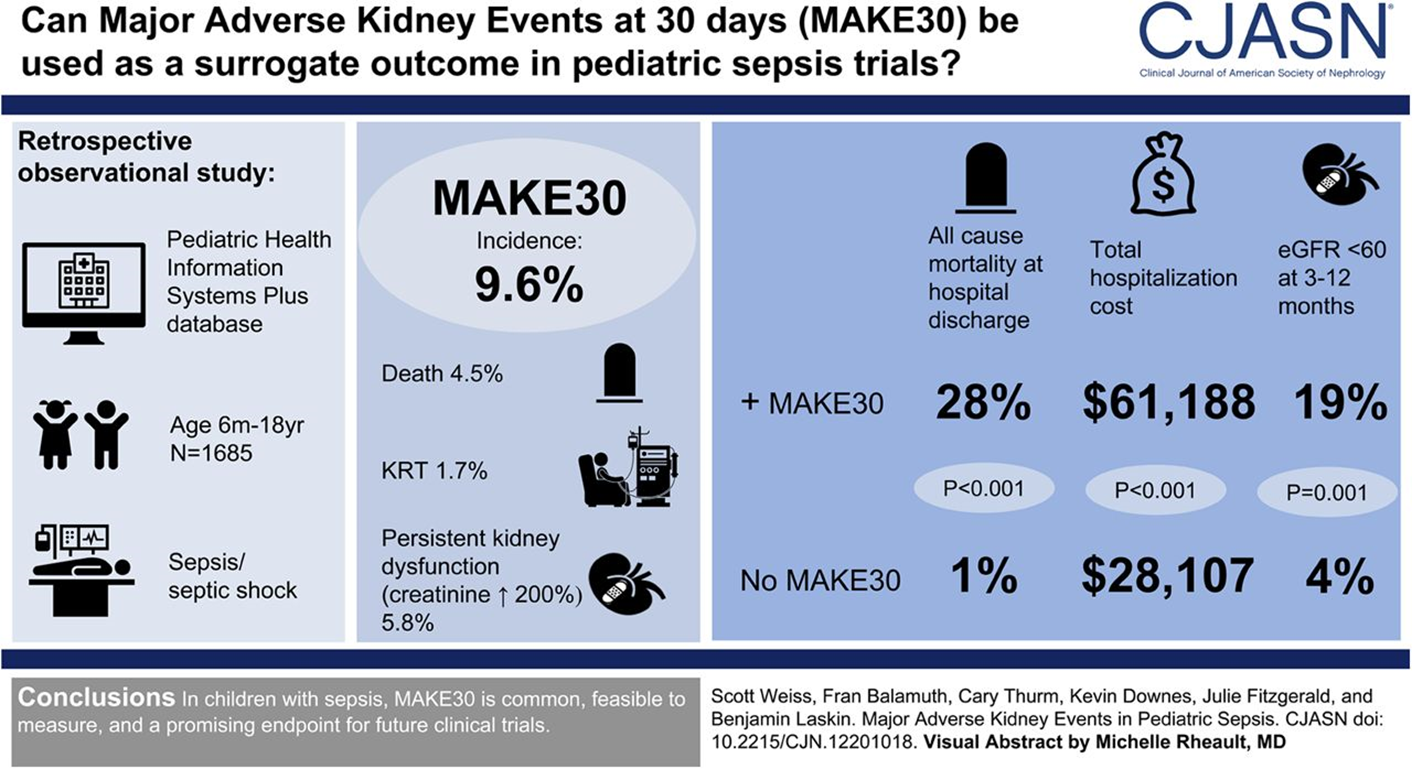
Figure1: From Scott L. Weiss et al. CJASN 2019;14:664-672
MAKE90 represents a medium-term outcome after AKI and may be the most appropriate endpoint as it is the time-point for diagnosis of CKD. One retrospective study showed the occurrence of at least one MAKE in a third of AKI survivors within a year. Recent studies now report the long-term outcomes of AKI as MAKE. In the ASSESS-AKI study which was a prospective matched cohort study, 1538 hospitalized patients with or without AKI who had survived 90 days after hospitalization were followed up for a median period of 4.7 years. 9% of this cohort developed progression of kidney disease which was defined as halving of GFR or development of ESKD. A study of this cohort reported a 36% overall incidence of MAKE at median follow-up. The definition of post-AKI CKD within MAKE is unclear with different studies using different percentages of decline in GFR as criteria. Development of CKD after AKI also increases the risk of MACE. These were grouped together with MAKE as MARCE (Major Adverse Renal and Cardiac Events) in a study done on the VA (Veterans Affairs) database. The AKI group was associated with higher risk of MARCE outcomes. It should be noted that much of the data about these outcomes of AKI are derived from high-income countries. There is paucity of data on incidence of MAKE from prospective studies in LMICs (Low and Middle Income Countries) where these events may contribute significantly to the future burden of chronic non-communicable disease in the community.
Risk factors for MAKE:
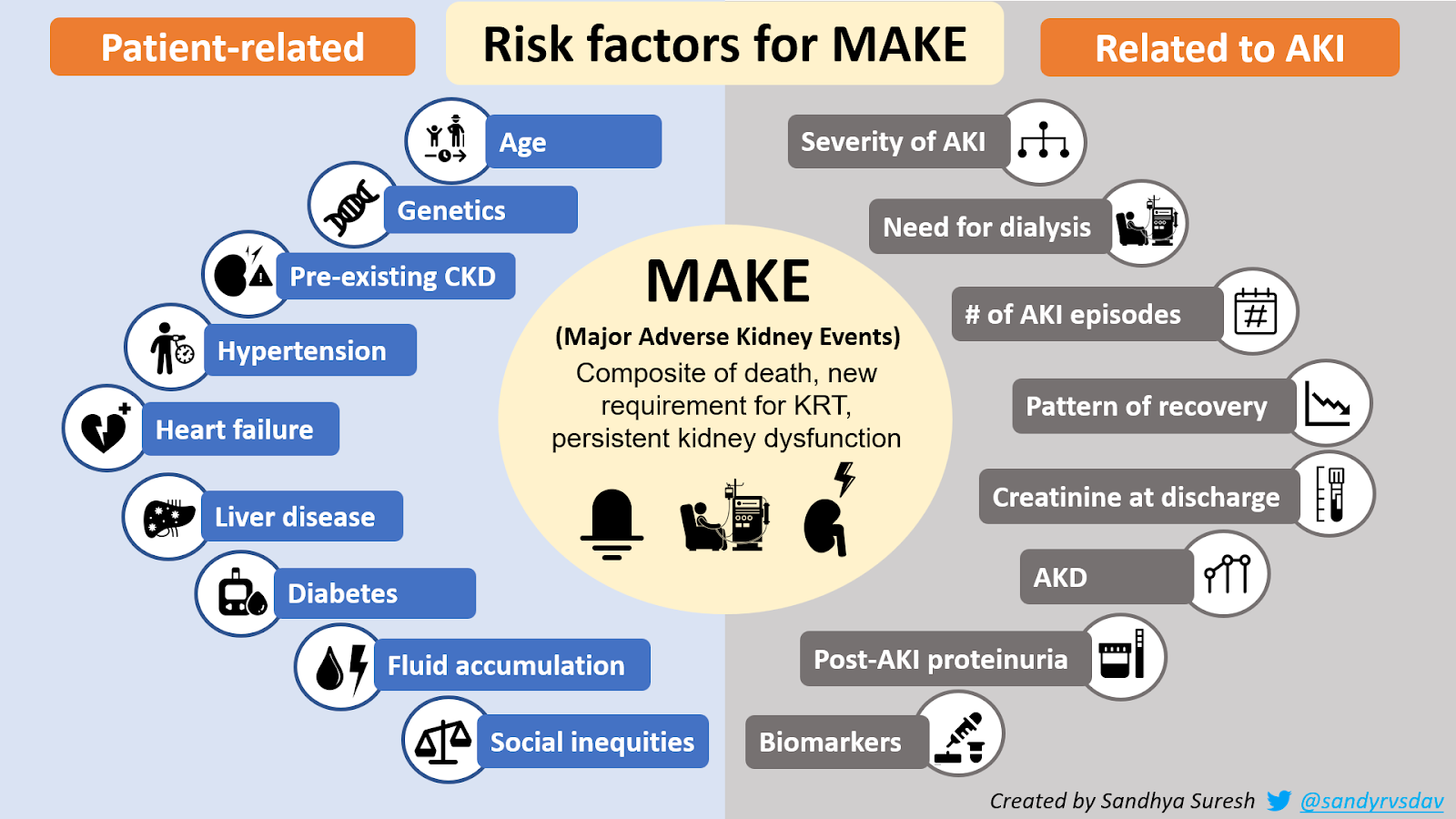
Figure 2: Risk factors for MAKE
Patient related risk factors:
Risk factors for the composite outcomes of CKD, ESKD and death after AKI include patient demographic factors, presence of underlying comorbidities and the severity of AKI as well as the degree of recovery. Aging and pre-existing CKD are associated with higher rates of adverse long-term outcomes due to greater susceptibility to the structural and functional changes that occur during AKI as the renal functional reserve is reduced in this population. Presence of comorbidities such as diabetes mellitus, hypertension and cardiovascular disease may be associated with pathophysiological changes in the kidneys causing glomerulosclerosis and tubulointerstitial disease thereby leading to glomerular hyperfiltration, proteinuria, reduction in residual renal function and accelerated progression of AKI to CKD. In one study, the Charlson Comorbidity index which predicts 10-year mortality risk of an individual based on presence of comorbidities was found to be a predictor of post-AKI CKD. Presence of hypertension, liver disease and congestive heart failure were also found to be associated with MAKE in the first year after an AKI. Genetic factors may modulate the risk of MAKE. For example, one study found an association between Aquaporin 5 polymorphisms and MAKE30 in patients with sepsis. Some studies have shown an association between cumulative fluid accumulation and MAKE30 outcomes in ICU patients with sepsis. However, it is unclear if the association is causal or only reflective of the severity of illness. Social factors such as race and ethnicity, income, environmental and living conditions have been shown to affect the entire spectrum of management of CKD from prevention to treatment. While the influence of these social determinants of health on the outcome of MAKE after an AKI episode have not been characterized, it is expected that social inequities would be a barrier to timely access to specialist care and adequate follow-up leading to higher incidence of the components of MAKE.
- AKI-related risk factors
Severity of AKI is an important predictor of progression to CKD with higher stages of AKI being associated with higher risk of Major Adverse Kidney Events at 1 year after AKI. Among AKI patients who required KRT (Kidney Replacement Therapy), MAKE occurred at a rate as high as 83% at the time of discharge to 93% at 3 years of follow-up. Repeated AKI episodes add to maladaptive repair with further nephron loss, glomerular hyperfiltration and tubulointerstitial fibrosis. In a study of diabetic patients with AKI, patients with 2 or more episodes of AKI had higher risk of development of CKD. A population based cohort study also showed increased risk of mortality with recurrent AKI. This study also demonstrated a 30% recurrence rate after the first episode of AKI and that each subsequent episode of AKI further increased the risk of a recurrent episode possibly due to loss of renal reserve, ongoing effects of the underlying disease and effect of therapies.
Recent evidence has focussed on the effect of timing and pattern of recovery of AKI on persistent renal dysfunction and other adverse outcomes. While there is a KDIGO classification for severity of AKI, there is no established stratification of AKI recovery patterns. The trajectory of renal function recovery after AKI may better reflect the pathophysiological process and response to therapy and has been shown to be predictive of short-term outcomes. The effect of renal recovery pattern on the incidence of MAKE was studied in the ASSESS-AKI cohort. Patients with AKI were categorized into resolving and non-resolving groups with resolving pattern defined by the decline of creatinine by ≥0.3mg/dl or by ≥25% within 72 hours. The risk of MAKE was significantly higher in the group with non-resolving pattern of renal recovery compared to the group with resolving pattern which in turn was greater than the group without AKI.
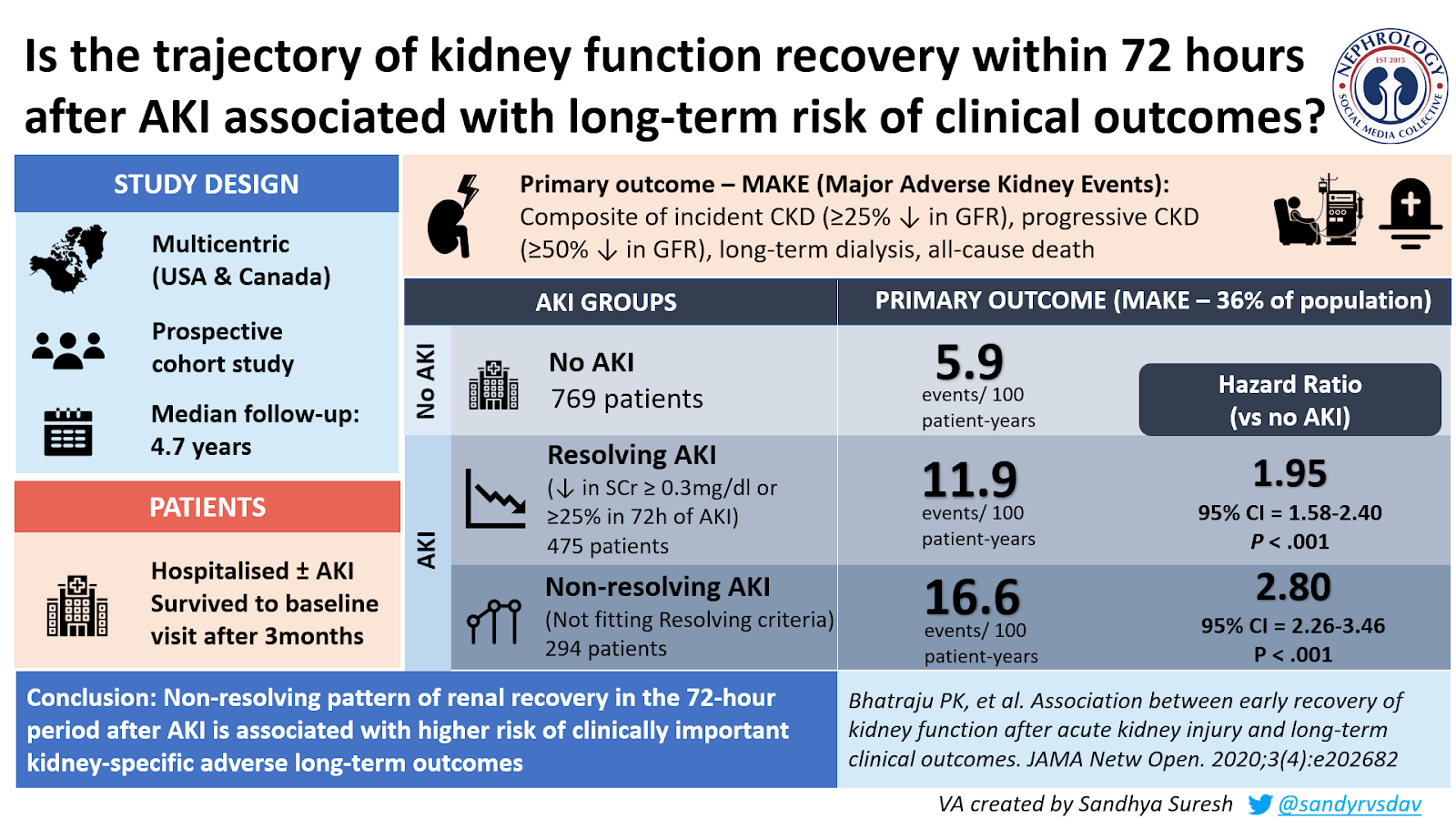
Figure 3: From Bhatraju et al, JAMA Netw Open. 2020;3(4);e202682
In another study by Kellum et al, the effect of trajectory of renal function was studied by dividing renal recovery in AKI stage 2 or 3 patients into 5 distinct phenotypes based on the presence or absence of early reversal (Absence of AKI for at least 24 hours within 7 days of AKI diagnosis) – sustained early reversal, reversal with relapse which recovered, relapse with no recovery, late reversal and no reversal. 1-year survival was significantly higher in the early reversal group at 90% compared to 40% in the group which had no renal recovery indicating that the pattern of recovery could predict the long-term outcome. Relapses were associated with 5-fold higher risk of mortality.
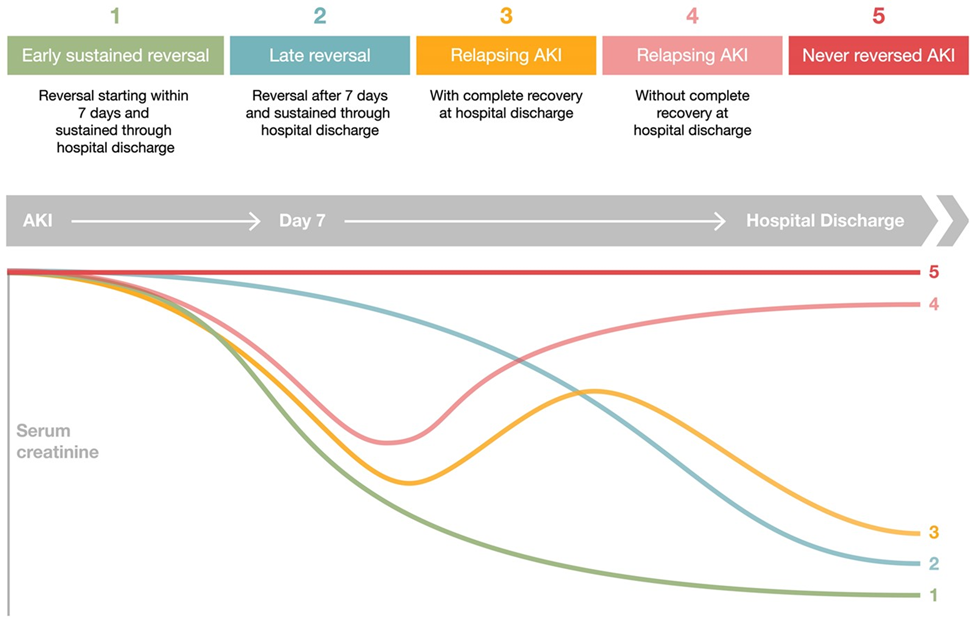
Figure 4: Phenotypes of AKI recovery. From Clin Kidney J, Volume 14, Issue 3, March 2021, Pages 789–804. Adapted from Kellum et al.
Studies on the effect of renal recovery on MAKE have been limited by different definitions used for recovery. The Acute Dialysis Quality Initiative (ADQI) defined recovery as return of creatinine to within 50% of baseline. ADQI also provided definitions for Acute Kidney Disease (AKD) to better describe the AKI-CKD continuum. While the ADQI criteria overestimated renal recovery, the criteria best associated with 3-year incidence of MAKE were found to be creatinine at discharge of either >30% or 0.4mg/dl above baseline or eGFR at discharge less than 70% of baseline value. The development of AKD (Acute Kidney Disease) was found to be a risk factor for the occurrence of MAKE regardless of the baseline eGFR with greater severity of AKD associated with higher risk of MAKE at 1 year. Post-AKI Urinary Albumin Creatinine ratio at 3 months was also found to be a significant predictor of progressive kidney disease indicating the importance of quantification of proteinuria after an episode of AKI in order to stratify risk of long-term outcomes. There is paucity of data on impact of modality and dose of KRT on the incidence of MAKE However, studies from the field of critical care nephrology are increasingly using short-term MAKE such as MAKE30 and MAKE-Discharge as endpoints in trials.
The role of biomarkers as predictors of MAKE after AKI is unclear. One study showed that early measurements of serum Cystatin-C and serum or urinary NGAL (Neutrophil Gelatinase-Associated Lipocalin) were significantly related to the incidence of MAKE at discharge and up to 1 year after the episode of AKI.
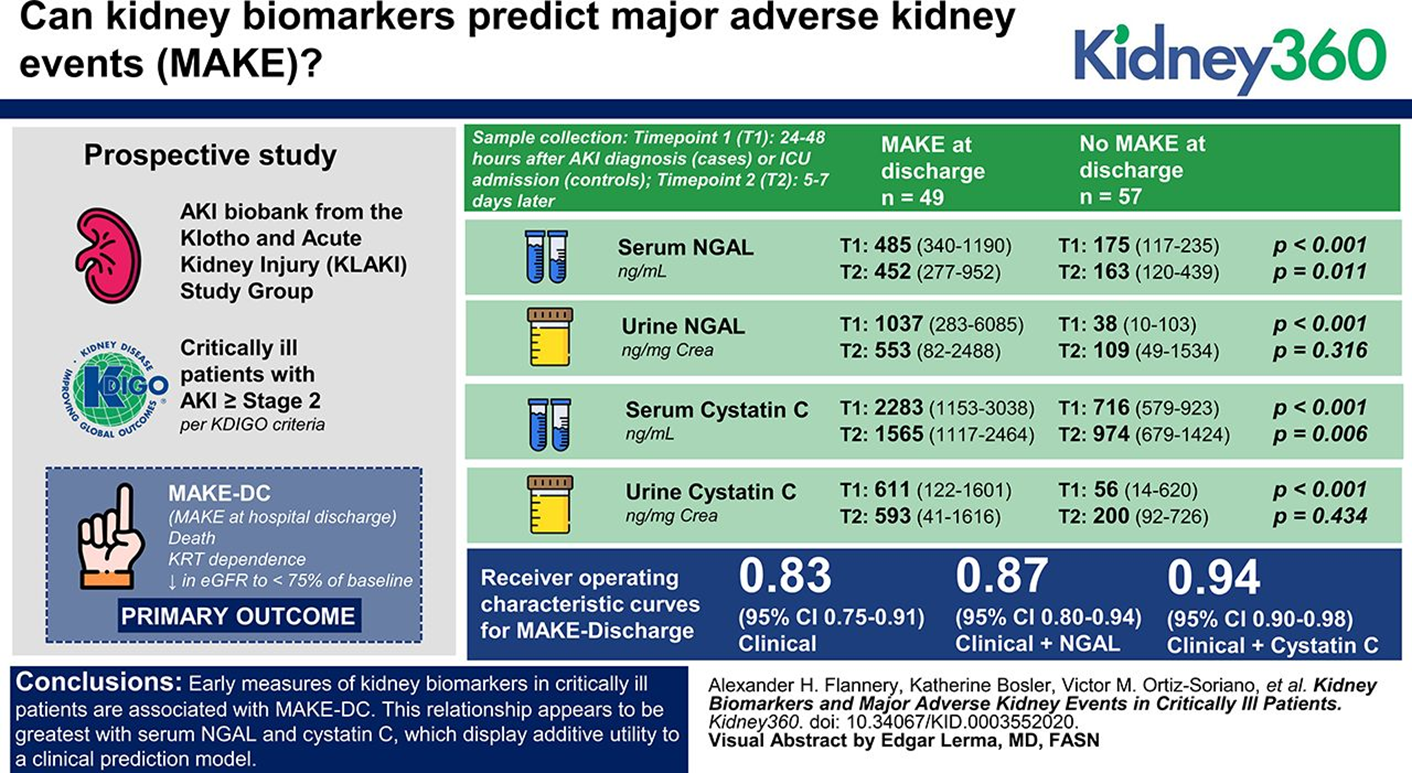
Figure 5: From Alexander H. Flannery et al. Kidney360 2021;2:26-32
Recently, studies such as the RUBY study and the FROG-ICU study have demonstrated the value of AKI biomarkers in predicting prognosis. Study of biomarkers in the progression of AKI to CKD may allow risk stratification as well as provide information on the ongoing pathophysiological processes in the AKI-CKD continuum thereby enabling the development of therapeutic interventions. The ADQI consensus statement recommends the incorporation of CKD biomarkers in the post-AKI setting.
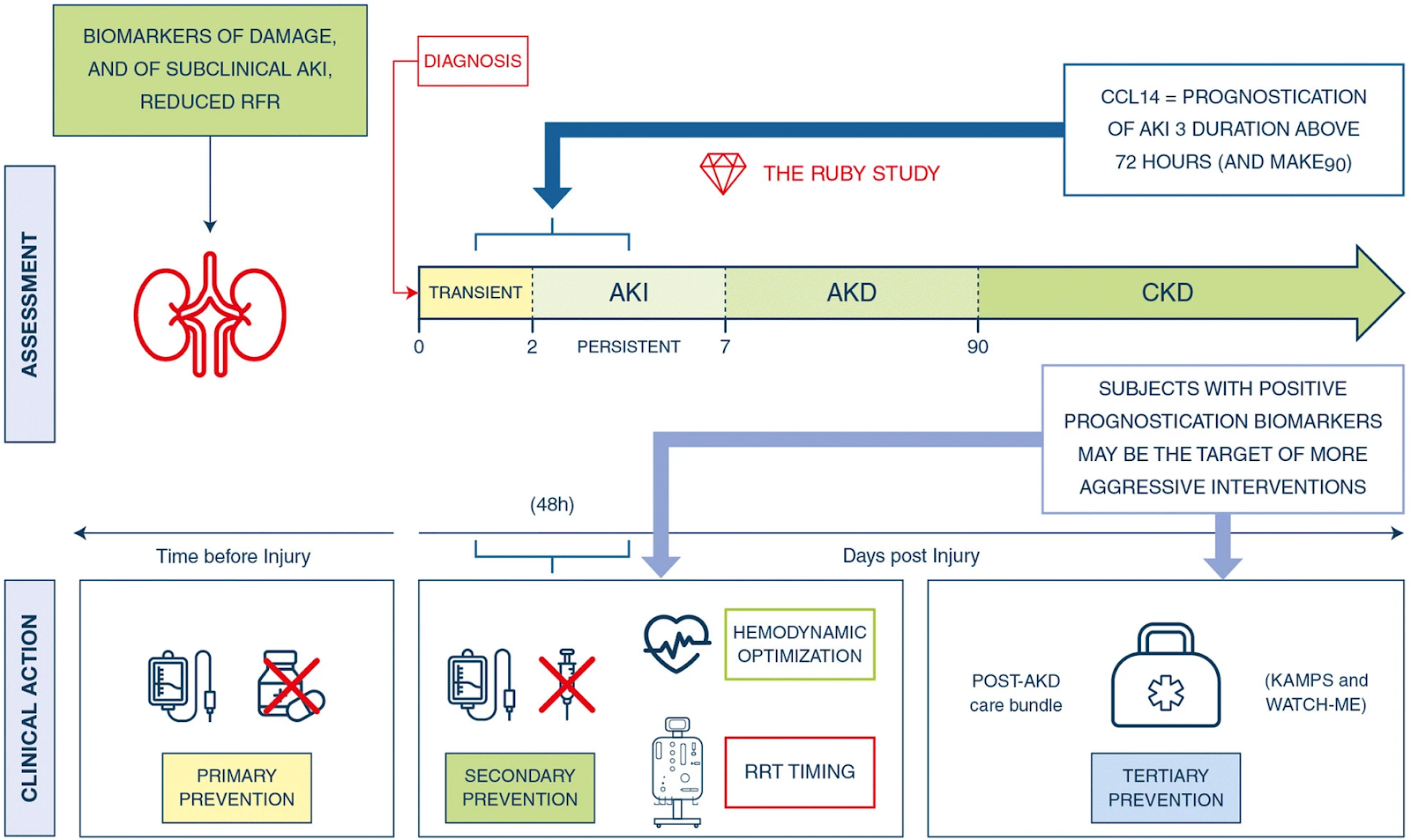
Figure 6: RUBY study and its implications
The SEA-MAKE score was developed based on a prospective study from ICUs in South East Asia and is a simplified scoring system of 9 different parameters to predict the development of MAKE28 in AKI patients. It had a sensitivity and specificity of 75% and 76% respectively at a cut-off value of 7.
Conclusion: MAKE is a clinically meaningful composite outcome which includes death, new requirement for KRT and persistent kidney dysfunction and is increasingly being used as an endpoint in AKI clinical trials especially in those determining the effectiveness of interventions. Short-term outcomes such as MAKE30 are preferred in critical care nephrology research as they are associated with increased event rates, reduced cost of the studies, and fewer patients lost to follow-up. Incorporation of MAKE90 as an outcome would be useful in trials studying the AKI-CKD transition. Longer-term MAKE endpoints at 1 year and beyond are reflective of the long-term impact of AKI on morbidity and mortality and could identify risk factors contributing to these outcomes as well as enable the study of interventions mitigating this risk.
Reviewed by Matthew A. Sparks

