 As usually happens when the renal fellows help with the medical student nephrology block, I found myself confronted last week with questions I couldn’t answer. One involved the pathophysiology of posterior urethral valves (PUV), which came up in a clinical case. In case there are other fellows who, like me, tend to avoid postrenal conditions in favor of studying more glamorous parenchymal diseases, here is a short primer on PUVS.
As usually happens when the renal fellows help with the medical student nephrology block, I found myself confronted last week with questions I couldn’t answer. One involved the pathophysiology of posterior urethral valves (PUV), which came up in a clinical case. In case there are other fellows who, like me, tend to avoid postrenal conditions in favor of studying more glamorous parenchymal diseases, here is a short primer on PUVS.In some senses, the name PUV is a misnomer, since using the word valve implies that there exists a functional valve somewhere, which in this case is dysfunctional. The “valve” in PUV is actually an overgrowth of urethral tissue that forms a membranous barrier to antegrade urine flow. Current thinking is that PUVs form in the embryonic period when there is abnormal integration of the mesonephric ducts into the posterior urethra.
There are three main types of PUVs, of which Type 1 comprises over 95% of cases. Ridges of membrane develop from the floor of the urethra, which then form membranous fins and extend anteriorly. You can see a good illustration of this on the right.

There is some debate as to whether there is a genetic component to this developmental anomaly, but there are no clear inheritance patterns. PUVs occur in boys only, and have an incidence rate of around 1/8,000 male births, but may be more common given increased likelihood of fetal demise. Clinically, they can be picked up on fetal ultrasound, where hydroureteronephrosis, a distended bladder, and a thickened bladder wall in utero can be seen. Postnatal complications include:
-pulmonary hypoplasia (a result of oligohydramnios)
-renal insufficiency, either due to obstructive uropathy or renal dysplasia
-urinary ascites (where high intraluminal pressure causes urine to extravasate from the kidneys)
In older children with a milder clinical course, voiding dysfunction can also be seen.
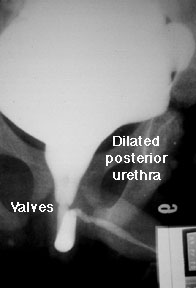
Definitive diagnosis is by VCUG, where bladder thickening, urethral dilation and severe vesicoureteral reflux are seen. Ultrasound may show hydronephrosis and possibly increased renal echogenicity. Treatment is initially to drain the bladder, and after medical stabilization, valve ablation. Long-term followup with urology, to address issues of chronic voiding dysfunction or incontinence, may be necessary. And for any irreversible kidney damage after relief of obstruction, enter the nephrologists.