There was a fascinating case published a couple of months ago in the American Journal of Medicine. I have a particular interest in this case as it was my clinic mentor, Julian Seifter, who made the diagnosis and published the case. I have waiting for a long time to write a post about it but couldn’t until the paper came out.
The case is a 50yr old man with a history of CKD, quadraplegia and an ileal conduit who was being investigated for CKD. His serum creatinine was 3mg/dl and a creatinine clearance was done to estimate his GFR. His urine creatinine concentration was 175mg and his calculated creatinine clearance was only 3 mls/min. At this point, RRT was recommended and the suggestion was that his serum creatinine overestimated his GFR because of reduced muscle mass.
However, because the urine creatinine still seemed inordinately low and he had no symptoms, an inulin clearance was done which revealed a true GFR of 21 ml/min. What could explain this discrepancy?
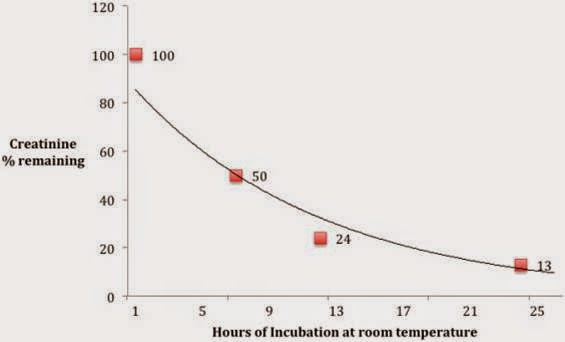
A urine culture grew diphtheroids, staphlococcus and streptococcus. Although creatinine, once it is produced in the muscle cannot be metabolized in humans, some bacteria produce creatininase and as a result are able to break it down. Corynebacterium is a diphtheroid that has been associated with the production of creatininase. Dr. Seifter suspected that there was a creatininase-producing bacterium in the ileal conduit that was metabolizing the creatinine leading to a falsely low creatinine clearance. To confirm this, he took a sample of the patient’s urine, added a known quantity of creatinine and incubated it for 24 hours at 20 degrees. The results are shown in the figure below.
Our GI tract has some creatininase-containing bacteria but under normal circumstances, the amount of creatinine clearance that they contribute is negligible – less than 2 ml/min GFR equivalent. However, in individuals with advanced CKD, both the relative and total clearance contributed by these GI bacteria increases such that in people with a GFR <10 the contribution of gut clearance can be as high as 4ml/min or approximately 50%. The opposite can also occur. The highest serum creatinine I ever saw was in a 50yr old woman with inflammatory bowel disease. She weighed 40kg but her admission creatinine was 38mg/dl. Despite this, she felt relatively well. She had previously undergone multiple bowel resections and had almost no functional bowel remaining. As a result, she had no gut clearance of creatinine and no upper limit to her serum creatinine concentration.
One final note, the urea clearance was not useful in the above patient either – his urine also contained urease – the clue to this was a very high urine pH (>9) in the presence of a mild metabolic acidosis and no history of RTA.

Fascinating case. Yhanks