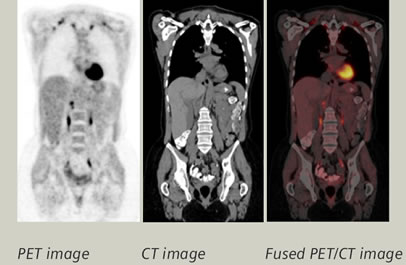
Positron emission tomography (PET)
is a nuclear imaging modality that provides functional imaging of structures
based on their ability to metabolize glucose and concentrate specific molecules
that have been labeled with a positron-emitting radionuclide. Metabolically
active cells (e.g, malignant or inflammatory) utilize and import more
glucose than other tissues and, thus, take up 18F-fluorodeoxyglucose (18F-FDG)
more avidly. Integrated PET/CT is preferred, because
it allows for more exact anatomic localization of isotope uptake and more accurate staging of cancers. PET is escaping oncology however
and starting to find a role in nephrology.
is a nuclear imaging modality that provides functional imaging of structures
based on their ability to metabolize glucose and concentrate specific molecules
that have been labeled with a positron-emitting radionuclide. Metabolically
active cells (e.g, malignant or inflammatory) utilize and import more
glucose than other tissues and, thus, take up 18F-fluorodeoxyglucose (18F-FDG)
more avidly. Integrated PET/CT is preferred, because
it allows for more exact anatomic localization of isotope uptake and more accurate staging of cancers. PET is escaping oncology however
and starting to find a role in nephrology.
In post-transplant
lymphproliferative disorders, integrated PET/CT is used as a measure
of disease activity. It has also been reported to differentiate fat-poor angiomyolipomas
from renal cell carcinoma with 94% sensitivity and 98% specificity. Integrated PET/CT
scanning may also be of utility in differentiating benign versus
malignant fractures and highlighting impending ones in patients with multiple
myeloma.
lymphproliferative disorders, integrated PET/CT is used as a measure
of disease activity. It has also been reported to differentiate fat-poor angiomyolipomas
from renal cell carcinoma with 94% sensitivity and 98% specificity. Integrated PET/CT
scanning may also be of utility in differentiating benign versus
malignant fractures and highlighting impending ones in patients with multiple
myeloma.
What about APKD? Cyst infection is common and may be
difficult to diagnose in the presence of sterile urine. Bobot et al
compared PET-CT to CT and MRI for a diagnosis of cyst infection. Cyst wall hypermetabolism was considered
as a positive PET-CT result. A diagnosis of cyst infection was made in 18 of 32
cases: 14 with positive PET-CT findings, and 4 false negatives. There were no
false positives and no hypermetabolism of cyst walls in 9 ADPKD control
patients. PET-CT had a sensitivity of 77%, a specificity of 100%, and a
negative predictive value of 77% compared to CT alone which had a sensitivity
of 7% and a negative predictive value of 35%. Radiation doses were comparable
and injection of nephrotoxic contrast was avoided in the former.
difficult to diagnose in the presence of sterile urine. Bobot et al
compared PET-CT to CT and MRI for a diagnosis of cyst infection. Cyst wall hypermetabolism was considered
as a positive PET-CT result. A diagnosis of cyst infection was made in 18 of 32
cases: 14 with positive PET-CT findings, and 4 false negatives. There were no
false positives and no hypermetabolism of cyst walls in 9 ADPKD control
patients. PET-CT had a sensitivity of 77%, a specificity of 100%, and a
negative predictive value of 77% compared to CT alone which had a sensitivity
of 7% and a negative predictive value of 35%. Radiation doses were comparable
and injection of nephrotoxic contrast was avoided in the former.
Similarly PET-CT may be useful the
detection of vasculitis in the large arteries with 29/35 patients with
known giant
cell arthritis showing active arterial inflammation (sensitivity >80%) . Patients suffering from granulomatosis polyangiitis (GPA) show
marked aortic
FDG uptake although it is unclear whether this is indicative of
atherosclerosis or large vessel involvement. If it is indeed the latter this calls
into question the traditional classification of vasculitis. FDG-PET/CT
accurately identified organ localizations in 16
patients with GPA, other than in nervous system, eye and skin, but may not
bring additional benefit to the usual organ screening.
detection of vasculitis in the large arteries with 29/35 patients with
known giant
cell arthritis showing active arterial inflammation (sensitivity >80%) . Patients suffering from granulomatosis polyangiitis (GPA) show
marked aortic
FDG uptake although it is unclear whether this is indicative of
atherosclerosis or large vessel involvement. If it is indeed the latter this calls
into question the traditional classification of vasculitis. FDG-PET/CT
accurately identified organ localizations in 16
patients with GPA, other than in nervous system, eye and skin, but may not
bring additional benefit to the usual organ screening.
Retroperitoneal fibrosis is a rare fibro-inflammatory
disorder that is most commonly idiopathic (>75%) and part of the
IgG4-disease related spectrum. PET-CT has emerged as a useful tool for the
assessment of disease activity and also detects any post-treatment residual
disease. It may lead to early diagnosis of relapses and may also detect diseased
sites other than the peri-aortoiliac tissue.
disorder that is most commonly idiopathic (>75%) and part of the
IgG4-disease related spectrum. PET-CT has emerged as a useful tool for the
assessment of disease activity and also detects any post-treatment residual
disease. It may lead to early diagnosis of relapses and may also detect diseased
sites other than the peri-aortoiliac tissue.
Could PET imaging have a role in the
detection of occult malignancy, inflammation or infection in secondary
glomerulonephritis? If we extrapolate from studies involving venous
thromboembolism (VTE), a prospective cohort of 99 patients with a first
episode of VTE reported occult cancer identified by PET/CT
in 23% of cases with a sensitivity and negative predictive value of 77% and 97%
respectively. However this sensitivity is still too low to justify its use as a
widespread screening tool in this capacity as nearly 1/4 cancers may be
missed.
detection of occult malignancy, inflammation or infection in secondary
glomerulonephritis? If we extrapolate from studies involving venous
thromboembolism (VTE), a prospective cohort of 99 patients with a first
episode of VTE reported occult cancer identified by PET/CT
in 23% of cases with a sensitivity and negative predictive value of 77% and 97%
respectively. However this sensitivity is still too low to justify its use as a
widespread screening tool in this capacity as nearly 1/4 cancers may be
missed.
Patients with ESRD undergoing
maintenance hemodialysis are highly susceptible to infections. Of 104
study patients, 73 (70.2%) had positive 18F-FDG PET/CT findings, and a
total of 95 major infection foci were identified. 7 (53.8%) of the 13 patients
with primary vascular access-related infections had concurrent metastatic foci.
28 patients (26.9%) had their treatments modified by PET/CT results. In this
population, positive PET/CT findings led to a significant change in clinical
management and independently predicted mortality.
maintenance hemodialysis are highly susceptible to infections. Of 104
study patients, 73 (70.2%) had positive 18F-FDG PET/CT findings, and a
total of 95 major infection foci were identified. 7 (53.8%) of the 13 patients
with primary vascular access-related infections had concurrent metastatic foci.
28 patients (26.9%) had their treatments modified by PET/CT results. In this
population, positive PET/CT findings led to a significant change in clinical
management and independently predicted mortality.
PET/CT may also help non-invasively prevent avoidable
transplant biopsies in kidney transplant recipients with suspected
antibody-mediated rejection. In 31
transplant recipients, PET/CT was performed in those who underwent biopsy
with a positive correlation between mean SUV and acute composite Banff score
(r2 =0.49). The area under the receiver operating characteristic curve was
0.93, with 100% sensitivity and 50% specificity using a mean SUV threshold of
1.6.
transplant biopsies in kidney transplant recipients with suspected
antibody-mediated rejection. In 31
transplant recipients, PET/CT was performed in those who underwent biopsy
with a positive correlation between mean SUV and acute composite Banff score
(r2 =0.49). The area under the receiver operating characteristic curve was
0.93, with 100% sensitivity and 50% specificity using a mean SUV threshold of
1.6.
But are there any side-effects or
limitations to use of PET-CT in our patients? For example, use of IV contrast
may be precluded in certain cases of renal impairment and this may impair the
optimal detection of small lung and liver lesions. IV contrast increases lesion
conspicuity, which is of particular importance in the evaluation of lesions
that do not always accumulate FDG. However use of PET-CT without IV contrast
has become more widespread and differentiation of benign from malignant lesions
is less relevant in Nephrology. The whole-body FDG distribution in patients on hemodialysis
may be different from those with normal renal function, because they lack
urinary FDG excretion and remain in a constant volume overload. There may be
significantly higher physiological FDG uptake in the soft tissues, spleen and
blood pool.
limitations to use of PET-CT in our patients? For example, use of IV contrast
may be precluded in certain cases of renal impairment and this may impair the
optimal detection of small lung and liver lesions. IV contrast increases lesion
conspicuity, which is of particular importance in the evaluation of lesions
that do not always accumulate FDG. However use of PET-CT without IV contrast
has become more widespread and differentiation of benign from malignant lesions
is less relevant in Nephrology. The whole-body FDG distribution in patients on hemodialysis
may be different from those with normal renal function, because they lack
urinary FDG excretion and remain in a constant volume overload. There may be
significantly higher physiological FDG uptake in the soft tissues, spleen and
blood pool.
In conclusion, I believe that
combined PET-CT imaging has the potential to be a very useful and versatile
tool for Nephrologists. Whether we are dealing with metastatic infections,
occult malignancy, suspicious GN or vasculitic relapses, it may be a revealing
diagnostic test at times when our concern exceeds the objective evidence that
we have to hand. That said, it is not without cost or risk, and therefore
should only be employed judiciously when likely to change clinical management.
combined PET-CT imaging has the potential to be a very useful and versatile
tool for Nephrologists. Whether we are dealing with metastatic infections,
occult malignancy, suspicious GN or vasculitic relapses, it may be a revealing
diagnostic test at times when our concern exceeds the objective evidence that
we have to hand. That said, it is not without cost or risk, and therefore
should only be employed judiciously when likely to change clinical management.
Post by Dearbhla Kelly,
NSMC Intern