His creatinine had risen from 1.1 on admission to 1.8 mg/dl. Urinalysis showed 3+ blood, 2+ protein, and trace leukocytes. Urine sediment showed 5-10 WBC, WBC casts and dysmorphic RBCs. He had no RBC casts, and no granular casts. He had a peripheral eosinophilia (2%). Urine eosinophils were negative. Serologies and complement levels were normal. Oxacillin was discontinued under the presumptive diagnosis of AIN secondary to beta-lactam antibiotics. Despite this intervention, his creatinine continued to rise and a renal biopsy was obtained. The biopsy results are shown below:
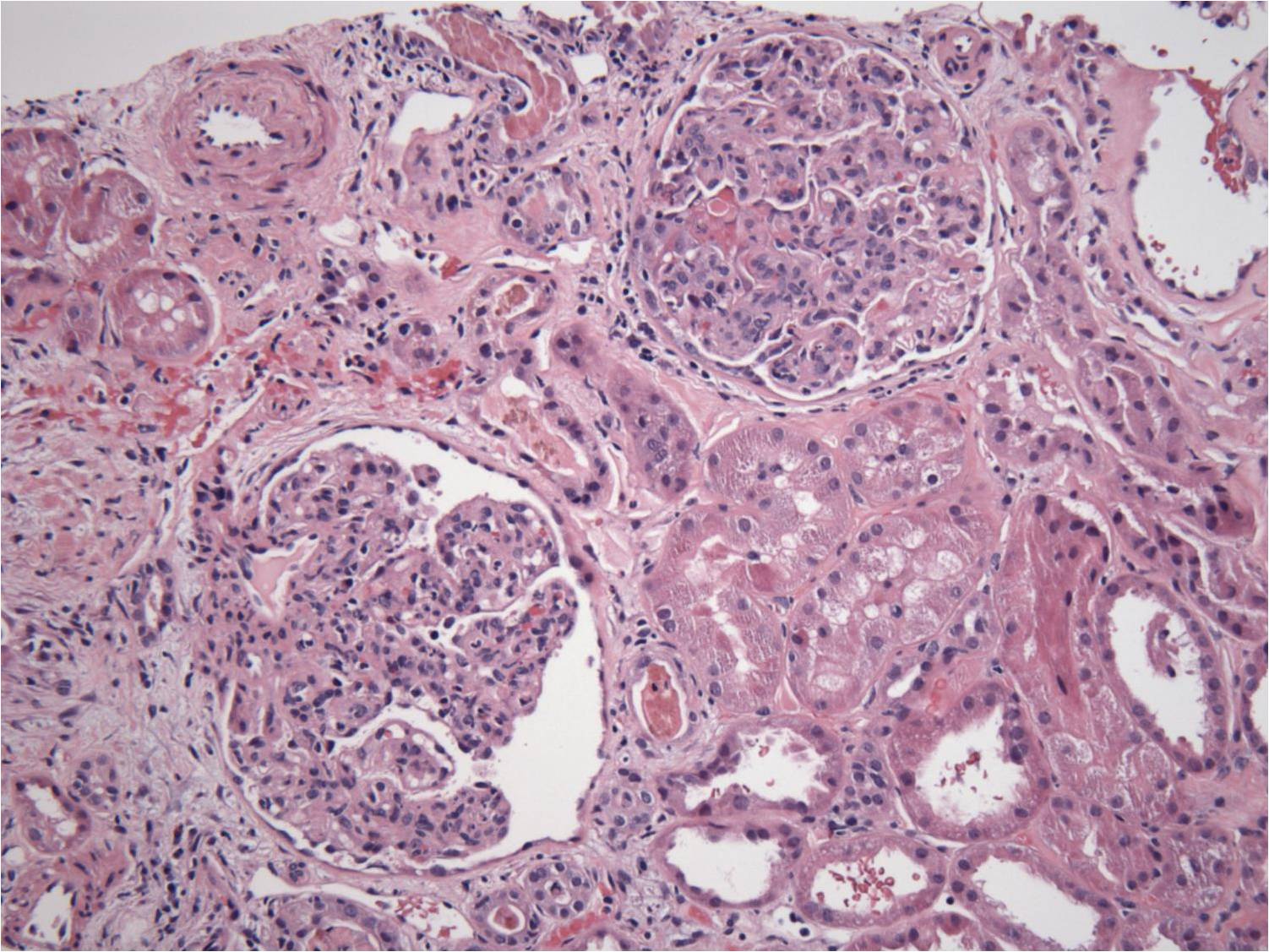
Two glomeruli with diffuse hypercellularity of the tuft. There is minimal interstitial inflammation
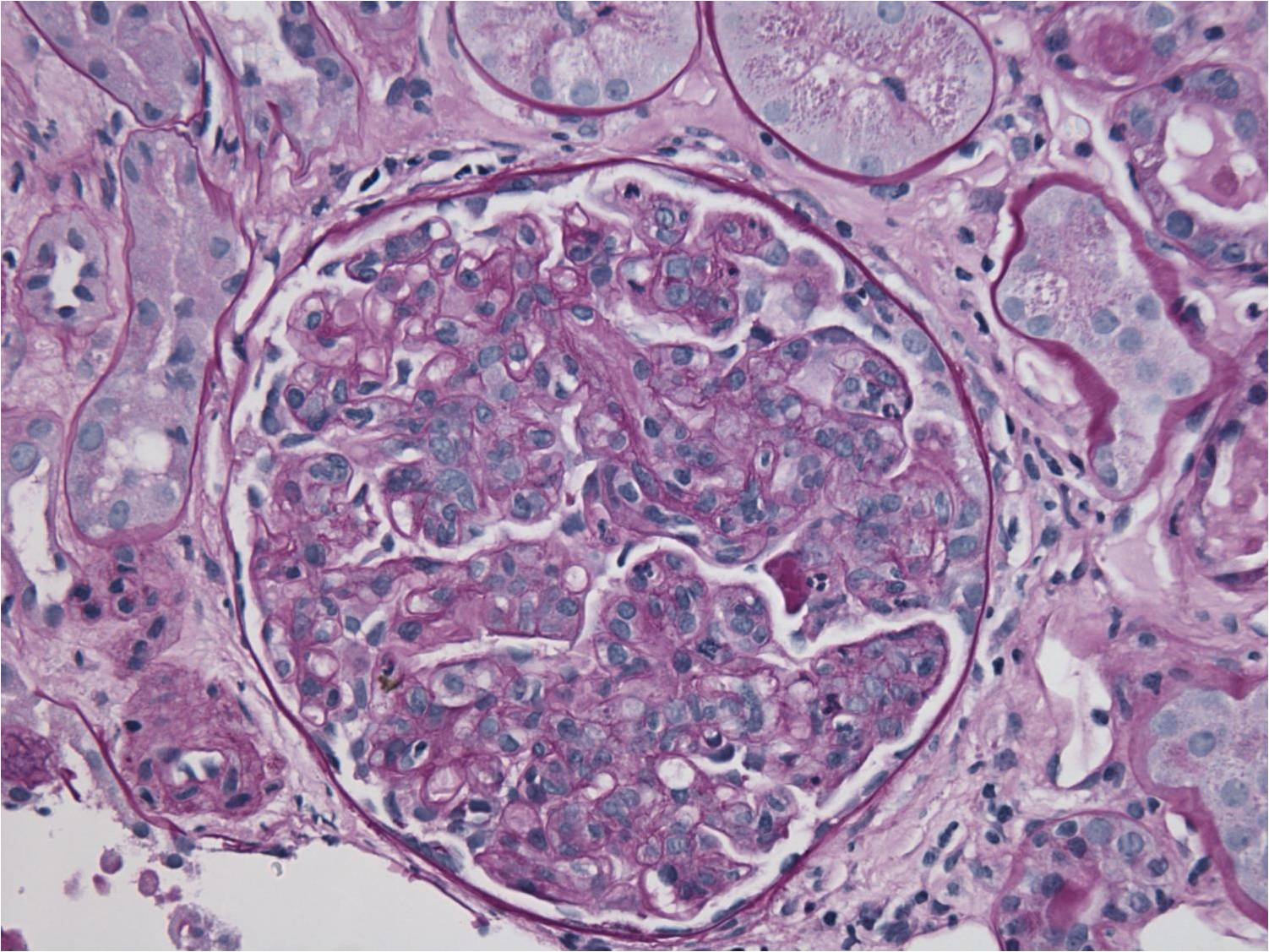
The infiltrating cells in the glomerular capillaries are predominantly mononuclear cells with isolated neutriphils.

Scattered deposits of IgG are noted along the peripheral capillary walls and in the mesangium.
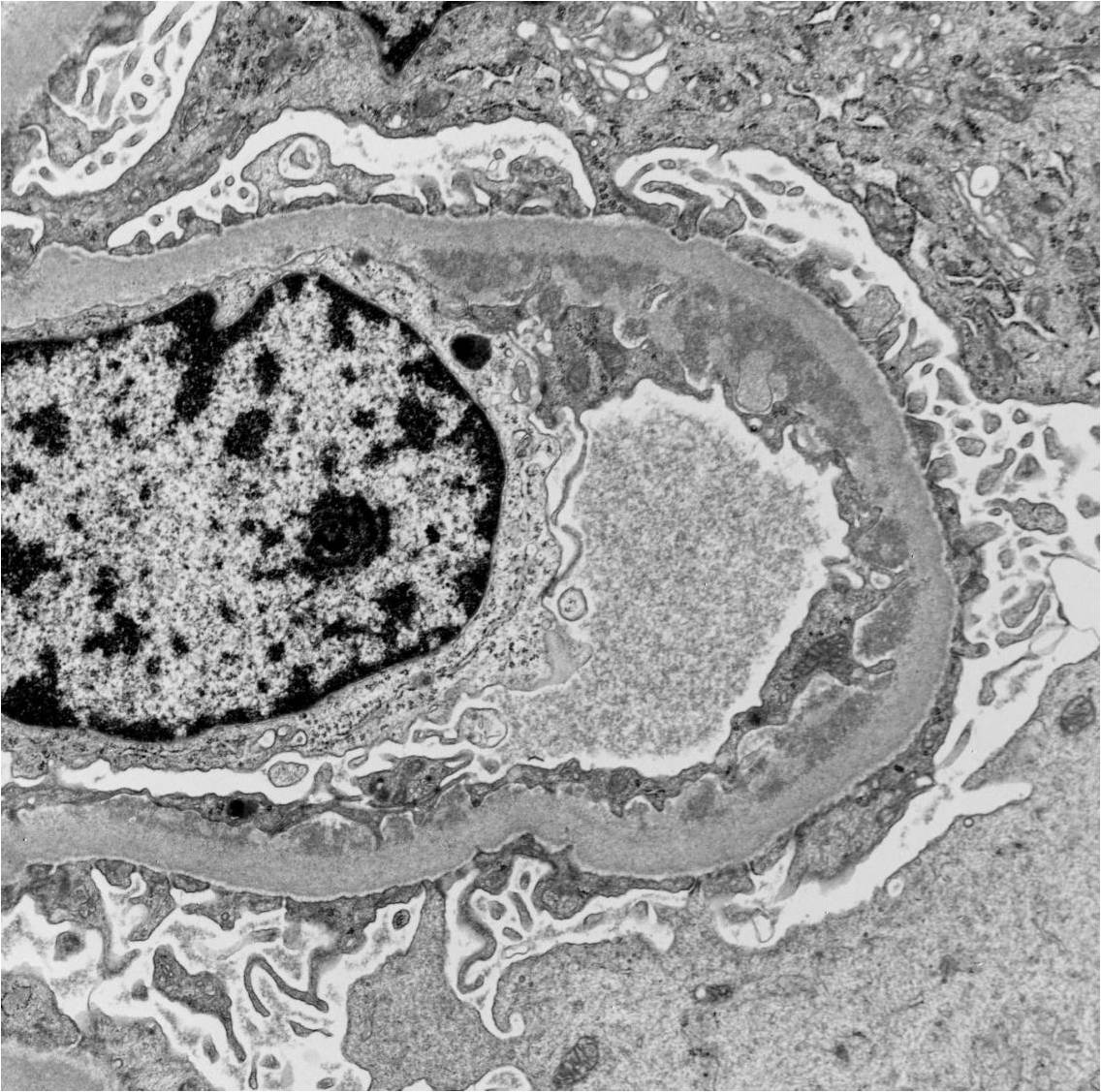
EM shows large and confluent subendothelial electron dense deposits.
Diagnosis: Diffuse proliferative glomerulonephritis, most likely post-infectioius and related to the patient’s sepsis.
This case appeared to be a relatively straight-forward case of AIN based on the exposure to a common culprit medication, the presence of eosinophilia and urinary white cell casts and the time course following admission. The presence of dysmorphic red cells was atypical although this is observer-dependent and there were no red cell cats which, while specific, are not very sensitive for the diagnosis of an acute GN. Traditional treatment comprising withdrawal of the offending medication and potential exposure to steroids may have been detrminetal in his case leading to inadequate treatment of his MSSA bacteremia.
The classic constellation of clinical signs in AIN is present in a minority of cases. For example, rash is present in ~15%, fever in 27%, eosinophilia in 23% and the triad in only ~10% of patients. White blood cell casts are sensitive but are a non-specific marker of intra-renal inflammation and are associated with a wide differential diagnosis. Urinary eosinophils are neither sensitive or specific and should not be used to make the diagnosis of AIN.
This case highlights the difficulty in making a clinical diagnosis of acute interstitial nephritis and the importance of a renal biopsy to confirm the clinical suspicion.
Posted by Katherine Garlo

