As
a child growing up in India, I have seen several family members performing
ritual fasting. Fasting is a
ubiquitous religio-cultural practice that is found, in varying forms, across
the world. The month-long Ramadan and Buddhist Lent fasts are examples of
religious observances practiced by followers of Islam, and Buddhism,
respectively. These fasts are characterized by a documented impact on metabolic health, which can be minimized by well-known management strategies.The practice of fasting
is a major part of Hinduism and can range from light restriction to
extreme abstention. Mahatma Gandhi was a fervent supporter of fasting by religious conviction and as a way of freeing
oneself of the constraints of the body. He used fasting as a means of exerting political
pressure and engaged in several hunger strikes to protest with
non-violence.
a child growing up in India, I have seen several family members performing
ritual fasting. Fasting is a
ubiquitous religio-cultural practice that is found, in varying forms, across
the world. The month-long Ramadan and Buddhist Lent fasts are examples of
religious observances practiced by followers of Islam, and Buddhism,
respectively. These fasts are characterized by a documented impact on metabolic health, which can be minimized by well-known management strategies.The practice of fasting
is a major part of Hinduism and can range from light restriction to
extreme abstention. Mahatma Gandhi was a fervent supporter of fasting by religious conviction and as a way of freeing
oneself of the constraints of the body. He used fasting as a means of exerting political
pressure and engaged in several hunger strikes to protest with
non-violence.

In
the western countries, starvation ketosis or ketoacidosis has been reported in
individuals with strict dieting (e.g.carb-restricted, ketogenic diets or Atkins diet), extreme exercise, and
rarely with malnutrition. Few cases of starvation-induced ketoacidosis during pregnancy and lactation, and during the perioperative period have also been reported in literature.
the western countries, starvation ketosis or ketoacidosis has been reported in
individuals with strict dieting (e.g.carb-restricted, ketogenic diets or Atkins diet), extreme exercise, and
rarely with malnutrition. Few cases of starvation-induced ketoacidosis during pregnancy and lactation, and during the perioperative period have also been reported in literature.
I
saw a young non-verbal woman with quadriplegia who was admitted from a nursing
home with a two-day history of worsening abdominal pain and leakage around her
percutaneous endoscopic gastrostomy
(PEG) tube site. Her medical history was significant for severe developmental
delay and chronic constipation. She was afebrile and the rest of the vitals
were stable. Her PEG tube feeds had been stopped one day prior to the hospital
admission due to abdominal pain. Additionally, she received small doses of iv
morphine for pain control. Due to no oral intake, she was maintained on
isotonic intravenous fluids.
saw a young non-verbal woman with quadriplegia who was admitted from a nursing
home with a two-day history of worsening abdominal pain and leakage around her
percutaneous endoscopic gastrostomy
(PEG) tube site. Her medical history was significant for severe developmental
delay and chronic constipation. She was afebrile and the rest of the vitals
were stable. Her PEG tube feeds had been stopped one day prior to the hospital
admission due to abdominal pain. Additionally, she received small doses of iv
morphine for pain control. Due to no oral intake, she was maintained on
isotonic intravenous fluids.
Laboratory blood work
revealed high anion gap metabolic
acidosis (HAGMA). I started going down the GOLDMARK mnemonic for differential diagnosis of
HAGMA to ascertain the cause.
revealed high anion gap metabolic
acidosis (HAGMA). I started going down the GOLDMARK mnemonic for differential diagnosis of
HAGMA to ascertain the cause.
Serum blood glucose,
lactate and salicylate levels were normal. Alcohol was not detectable in serum,
and there was no known exposure to any toxins. Osmolal gap was not elevated.
Urine pregnancy test was negative. Urine analysis showed significant
ketonuria. Serum beta-hydroxybutyrate was negative.
lactate and salicylate levels were normal. Alcohol was not detectable in serum,
and there was no known exposure to any toxins. Osmolal gap was not elevated.
Urine pregnancy test was negative. Urine analysis showed significant
ketonuria. Serum beta-hydroxybutyrate was negative.
After ruling out the common causes of acute metabolic
acidosis (lactic acidosis, diabetic ketoacidosis, drug-induced ketoacidosis,
ingestion of toxic alcohols, uremia, and acute kidney injury), we
concluded starvation ketosis was the cause of HAGMA due to elevated urinary
ketone levels.
acidosis (lactic acidosis, diabetic ketoacidosis, drug-induced ketoacidosis,
ingestion of toxic alcohols, uremia, and acute kidney injury), we
concluded starvation ketosis was the cause of HAGMA due to elevated urinary
ketone levels.
In
clinical practice, fasting or starvation is seldom suspected to be the cause of
significant metabolic ketoacidosis. Ketone bodies, which are water-soluble,
fat derived fuel are produced by the
liver during the time of glucose deficiency. These ketone bodies are used by body tissues for energy
generation, when there is limited glucose availability. Additionally,
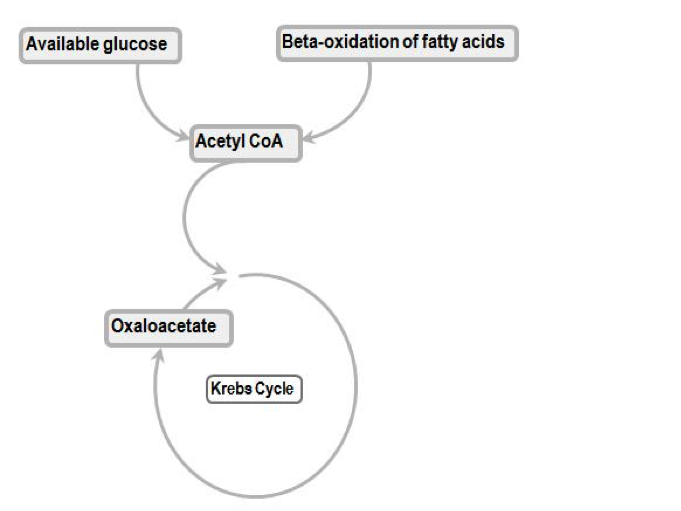
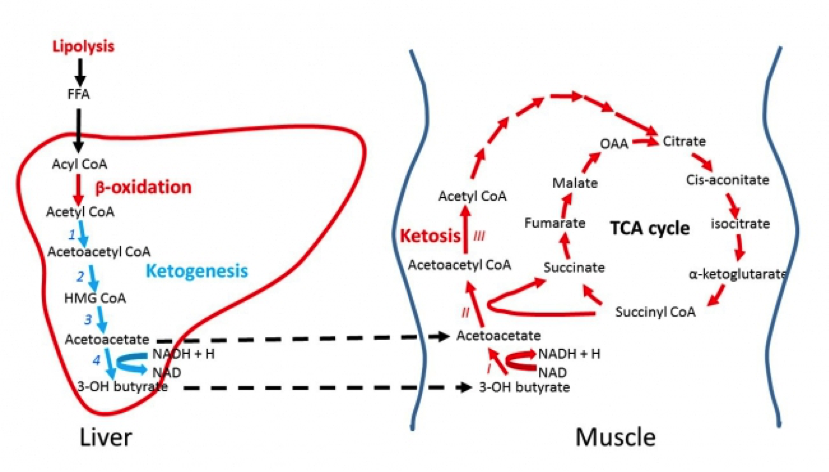
starvation results in decreased insulin and increased lipolysis. The resulting
increase in the delivery of free fatty acids to the liver exceeds the capacity
of acetyl-CoA to enter the Krebs cycle,which is then diverted into ketogenesis.
In otherwise healthy individuals, mild ketosis (ketoacid concentration of about 1 mmol/L) develops
generally after 12-14 hours of fasting and arterial pH remains
above 7.3.
clinical practice, fasting or starvation is seldom suspected to be the cause of
significant metabolic ketoacidosis. Ketone bodies, which are water-soluble,
fat derived fuel are produced by the
liver during the time of glucose deficiency. These ketone bodies are used by body tissues for energy
generation, when there is limited glucose availability. Additionally,
starvation results in decreased insulin and increased lipolysis. The resulting
increase in the delivery of free fatty acids to the liver exceeds the capacity
of acetyl-CoA to enter the Krebs cycle,which is then diverted into ketogenesis.
In otherwise healthy individuals, mild ketosis (ketoacid concentration of about 1 mmol/L) develops
generally after 12-14 hours of fasting and arterial pH remains
above 7.3.
Since the degree of ketoacidosis usually remains
relatively mild, the term “ketosis” is typically used rather than
“ketoacidosis.” But
starvation combined with physiological stress can lead to increased anion gap
and ketoacidosis.This
usually occurs when there is a relatively large glucose requirement, as occurs
with fasting in the very young (eg, normal neonates generally have some degree
of ketosis for several days), or in pregnant or lactating women.
relatively mild, the term “ketosis” is typically used rather than
“ketoacidosis.” But
starvation combined with physiological stress can lead to increased anion gap
and ketoacidosis.This
usually occurs when there is a relatively large glucose requirement, as occurs
with fasting in the very young (eg, normal neonates generally have some degree
of ketosis for several days), or in pregnant or lactating women.
Our patient was
started on a D5-half NS drip. Following an exchange of her PEG tube, feeding
was restarted. The metabolic acidosis resolved within two days and the patient was
discharged back to the nursing home. This was a great learning case for me. It
is consults like these that make nephrology so challenging and exciting!
started on a D5-half NS drip. Following an exchange of her PEG tube, feeding
was restarted. The metabolic acidosis resolved within two days and the patient was
discharged back to the nursing home. This was a great learning case for me. It
is consults like these that make nephrology so challenging and exciting!
Post by Manasi Bapat, nephrology fellow at Icahn School of Medicine,
Mount Sinai, NY and NSMC Intern 2018
Mount Sinai, NY and NSMC Intern 2018

Agreed that’s an interesting case I had one case of starvation ketosis in a pregnant woman with severe hyper emesis during the first term. I was able to correct ot by giving dextrose containing fluids. In your case interesting that the beta hydroxybutrate is negative. Do you have any other information as to why this would be