Donor specific Antibodies (DSA) are one of the established biomarkers for predicting antibody mediated rejection (ABMR). This blog is a short synopsis on DSA and their complex characteristics in kidney transplantation.
The main sensitizing events include organ transplant itself pregnancies and blood transfusions. It is important for the clinician to take the history of shared children with a partner who is a potential live donor. Sensitization is generally represented as the % panel reactive antibody (PRA), the proportion of a representative population that the recipient has anti-HLA antibodies to. This also estimates the likelihood of a positive cross match to potential donors.
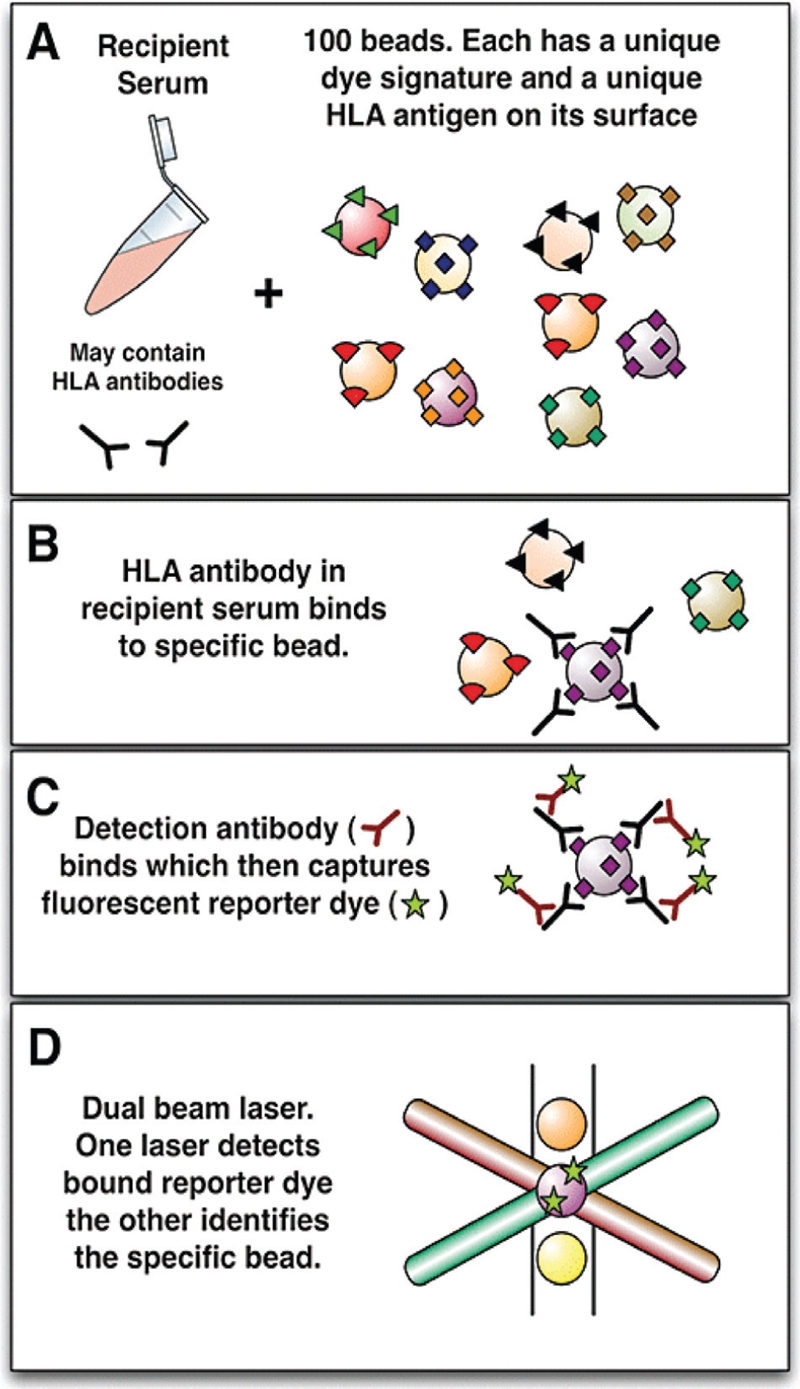
We have come a long way from the less sensitive complement based cytotoxic assays and ELISA to the newer and more sensitive multiplexed particle based flow cytometry (e.g. Luminex, see image). The newest kid on the block of sensitive testing for DSA is next generation sequencing (NGS). Single bead antigens assessed on a Luminex platform can identify the precise antibody present. This information is used in identifying preformed antibodies against a potential donor on a virtual cross match (so called because single antigen beads are added to recipient serum, without donor cells being involved). When ABMR is suspected, the presence of de-novo DSA or rising titers of pre-existing DSA contributes to the diagnosis.
De-novo DSA can develop in 30% of transplant recipients who were previously not sensitized. De-novo DSA mainly develop against HLA Class II antigens (often DQ). The risk factors for de-novo DSA formation include:
- High HLA mismatches (especially DQ).
- Inadequate/non adherence to immunosuppression.
- Graft inflammation which leads to increased immunogenicity (viral infections like CMV, cellular rejection episodes or ischemic injury).
Importance of DSA class & IgG Subclass
DSA target specific epitopes in the polymorphic regions of the HLA antigens (see NephMadness for more on epitopes/eplets).
HLA Class I: A,B,C antigens; present on all nucleated cells, one alpha chain and a beta2-microglobulin; epitopes located on the polymorphic alpha chain.
HLA Class II: DR, DQ, DP; present on all antigen-presenting cells, one alpha & 1 beta chain; both chains are polymorphic.
|
IgG1
|
IgG2
|
IgG3
|
IgG4
|
|
Complement binding
Most abundant
|
Weakly complement binding
|
Complement binding (best)
Mainly associated with acute ABMR
|
Does not bind complement at all
Biomarker of mature alloresponse and chronic graft injury
|
Class I antibodies are usually of IgG1 or IgG3 subclass so are usually complement binding. They are unusally associated with acute ABMR and graft loss. Class II antibodies are usually IgG2/4 subclass and are usually detected late and are not complement binding. Usually quite persistent and associated with chronic injury.
Usually expressed as the Mean Fluorescence Intensity (MFI) on the solid phase (single bead) assay. There is no standardisation currently and each transplant center develops their own cut-offs. Important points to consider regarding DSA strength (see NephMadness for more): (i) Prozone effect: False negative or low titers may occur despite high levels of antibody in the presence of inhibitors (serial dilutions help mitigate prozone effect). (ii) DSA against shared epitopes may be diluted across the beads giving lower individual MFI.
Relationship between DSA and C4d deposition in the kidney
C4d is the degradation product of the classic complement pathway. It binds covalently to the endothelial basement membrane. Positive C4d staining in peritubular capillaries serves as an immunological foot print of ABMR – seen as a linear pattern best seen in frozen tissue section. It is important to note that not all ABMR will be C4d positive and that isolated C4d positivity may not portend a bad prognosis (graft accommodation in ABO incompatible transplantation is a well known example).
Post by Rajeeva Parthasarathy


Thanks for the very important notes. Salient points are well highlighted.
Succinct teaching points as always.
I appreciate your effort in making one’s understanding easier .
Thanks