One of the things that I always highlight when teaching fellows and residents is the importance of appropriate drug dosing for patients on dialysis and one of the drugs that is most often inappropriately dosed in my experience is gabapentin. Today, an article in JASN highlights again the importance of not overusing this drug in the dialysis population.
Gabapentin and pregabalin are often used in patients with CKD primarily to treat neuropathic pain and restless leg syndrome and given the high prevalence of diabetes in this population, the proportion who receive these drugs is very high. In patients with normal renal function, the maximum dose of gabapentin is 3600mg daily in divided doses. However, gabapentin is renally cleared and so the dose needs to be adjusted according to the GFR. For patients on dialysis, the recommended dose is 100-300mg post dialysis on dialysis days only. However, this is routinely exceeded in clinical practice.
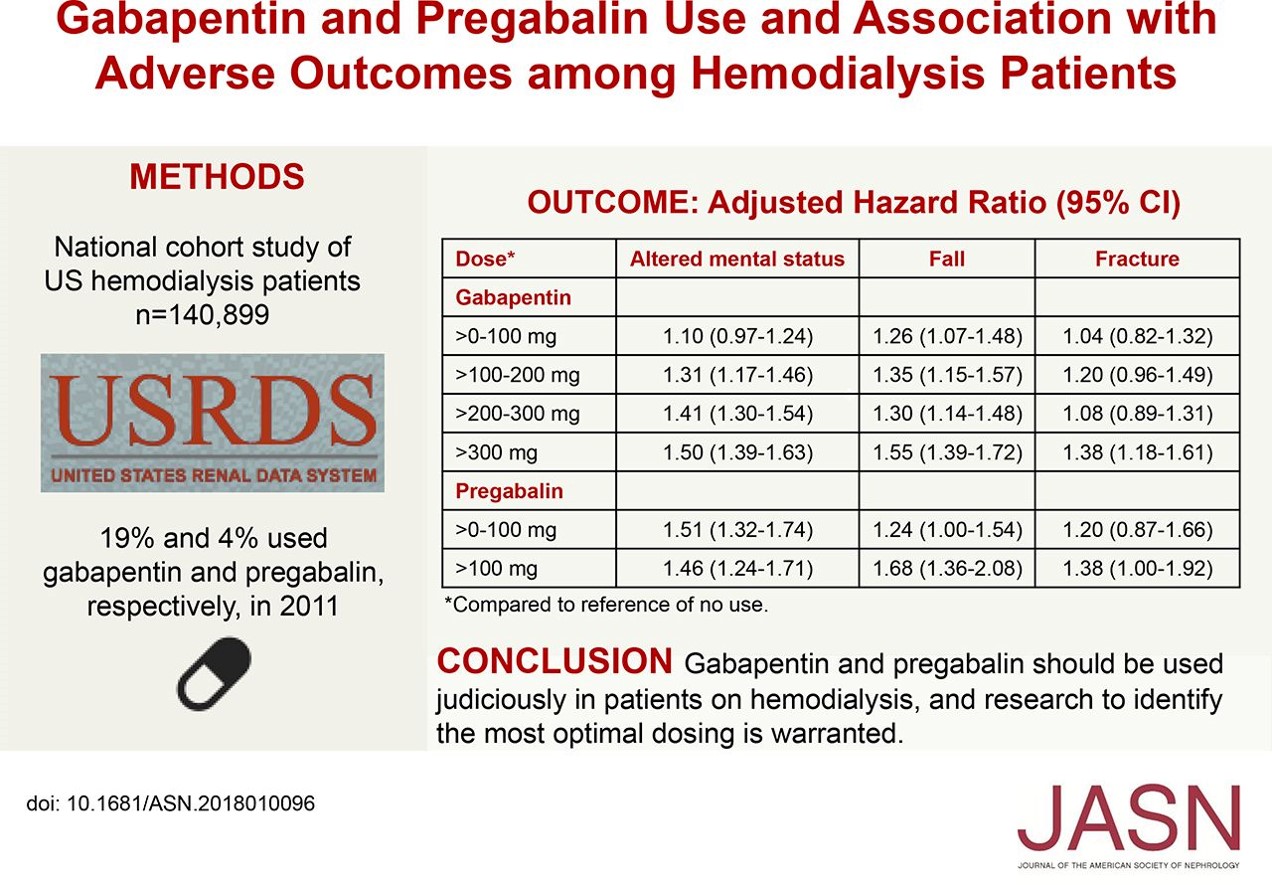
The study in JASN looked at medicare prescriptions for gabapentin and pregabalin in dialysis patients examined the relationship between the doses used and a variety of outcomes including altered mental status, falls and fractures. 20% of the dialysis population received at least one prescription for these drugs in 2011. Even at the lowest doses (less than 300mg daily), there was an association between the use of these drugs and AMS and falls while doses greater than 300mg daily were associated with a 40% increase in the risk of fracture. Similar results were found for the higher doses of pregabalin.
Of course, this was an observational study and there may have been unmeasured confounders that may have biased the results but the authors did account for other medications that can increase the risk of falls.
Overall, this should serve as a reminder to the community that we need to more carefully police the dosing of medications in our dialysis population, particularly when they are admitted to hospital.

