Last week we looked at the basics and useful terminology employed for examining a vascular access. Now we will focus on specifics of the physical exam.
Physical Examination
Inspection (Look)
Visual inspection can provide important clues regarding the cause of AV access dysfunction. Inspect the AVF or AVG to determine its configuration and length, while also assessing for abnormalities such as aneurysms/pseudoaneurysms, collateral veins, signs of hand ischemia (cyanotic fingers, hand pallor), or signs of infection (erythema, purulent drainage). It is important to compare the AV access extremity with the contralateral extremity for asymmetry or collateral veins. Similarly, the head, neck, chest and face should be inspected for swelling or collateral veins.
| Finding | What It Suggests |
| Head: Facial edema | Superior vena cava stenosis |
| Neck: Scars (prior central venous catheters) | Increased risk of central venous stenosis |
| Chest: Edema Breast swelling Collateral veins Implantable devices | Central vein stenosis Central vein stenosis Central vein stenosis Increased risk of central vein stenosis |
| Arm: Edema Collateral vein(s) Aneurysms and pseudoaneurysms Visible pulsation | Central vein stenosis Stenosis near the vein(s) Outflow stenosis Outflow stenosis |
| Hand: Cyanosis,pallor, skin necrosis, or dystrophic nails | Vascular steal syndrome |


Figures 5 & 6. Aneurysmal fistulas with a shiny central erosion. From Atlas of Dialysis Vascular Access.

Figure 7. Pseudoaneurysmal AV graft. From Atlas of Dialysis Vascular Access.
| Clinical Pearl: True aneurysms are dilations involving the entire vessel wall, whereas pseudoaneurysms are dilations secondary to hematomas that occur at sites of repetitive cannulation. Unlike true aneurysms, pseudoaneurysms are not covered by the vessel wall. Glassy, thin skin or presence of ulceration over an aneurysm or pseudoaneurysm requires urgent surgical evaluation, due to high risk of AV access rupture . |

Figure 8. Cyanotic fingertips, consistent with vascular steal syndrome. From Atlas of Dialysis Vascular Access.

Figure 9. Marked right arm swelling due to ipsilateral central vein stenosis. From Atlas of Dialysis Vascular Access.
The arm elevation test is a simple method to diagnose outflow vein stenosis. Under normal circumstances, when the fistula arm is raised above the level of the heart, the fistula will collapse. If an outflow stenosis is present, the area of the fistula distal to the stenosis will remain distended. Note: this test works best with forearm AVFs and is not valid for AVGs. Patients can be taught to perform the arm elevation test as a way to self-monitor their AV accesses. (Click here for a video demonstration of the arm elevation test.)
Palpation (Feel)
A normal thrill has two components: a gentle, continuous (systolic and diastolic) vibration over the length of the AV access and a soft pulsation. The thrill is best felt with the palm of the hand. Stenotic lesions intensify the thrill over the area of stenosis and lead to loss of the diastolic component. An extremely strong (“water-hammer”) pulse over an AV access is concerning for venous outflow stenosis. Weak pulsation suggests a problem with the inflow. In an AV graft, it is normal to feel a strong thrill at the arterial anastomosis that diminishes slightly as you move closer to the venous outflow
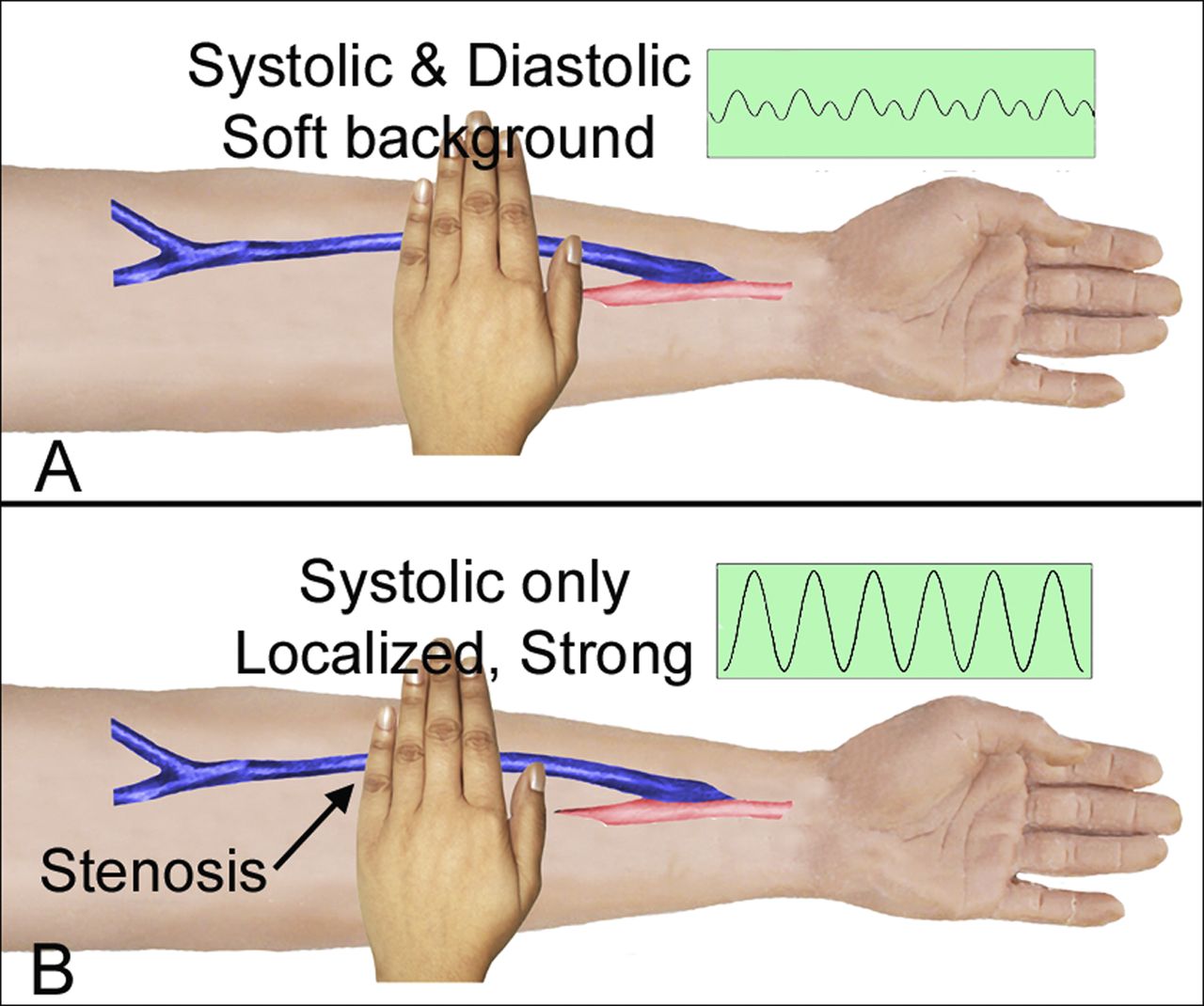
Figure 10. Palpation of an AV access is best done using the whole hand. In the absence of a stenotic lesion, the thrill is continuous (A). The thrill becomes stronger and loses its diastolic component if a stenosis is present (B). From Salman and Beathard, CJASN, 2013.
The pulse augmentation test is used to evaluate the inflow. The AV access is completely occluded several centimeters above the arterial anastomosis with one hand, while the other hand is used to assess the quality of the pulse. Increased pulse intensity (augmentation) with occlusion of the outflow vein is a normal finding. Failure of the pulse to augment when the outflow vein is occluded suggests the presence of inflow stenosis.
The pulse augmentation test may also be used to assess the direction of blood flow in an AVG. When the center of the AVG is occluded, the side with an intensified pulse is the portion of the AVG that is connected to the artery, while the side without pulsation is the portion of the AVG connected to the vein.
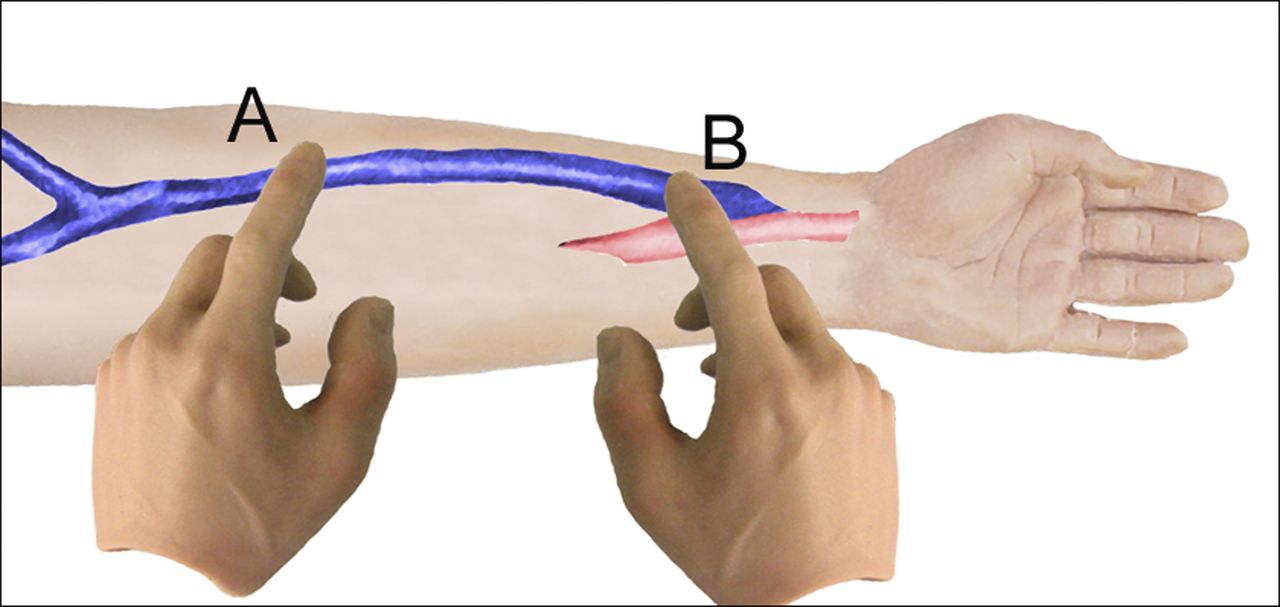
Figure 11. The augmentation test. The left hand (A) is used to occlude access outflow while the right (B) is used to assess the intensity of the pulse. From Salman and Beathard, CJASN, 2013.
The sequential occlusion test is used to determine the presence of collateral veins. Similar to the pulse augmentation test, one hand is used to occlude the AV access outflow while the other hand is used to palpate the thrill. The AV access is occluded progressively further down the venous outflow tract. If no collateral vein is present, no thrill will be felt. However, if a thrill is palpable despite occlusion of the AV, that indicates the presence of a collateral vein below the point of occlusion.
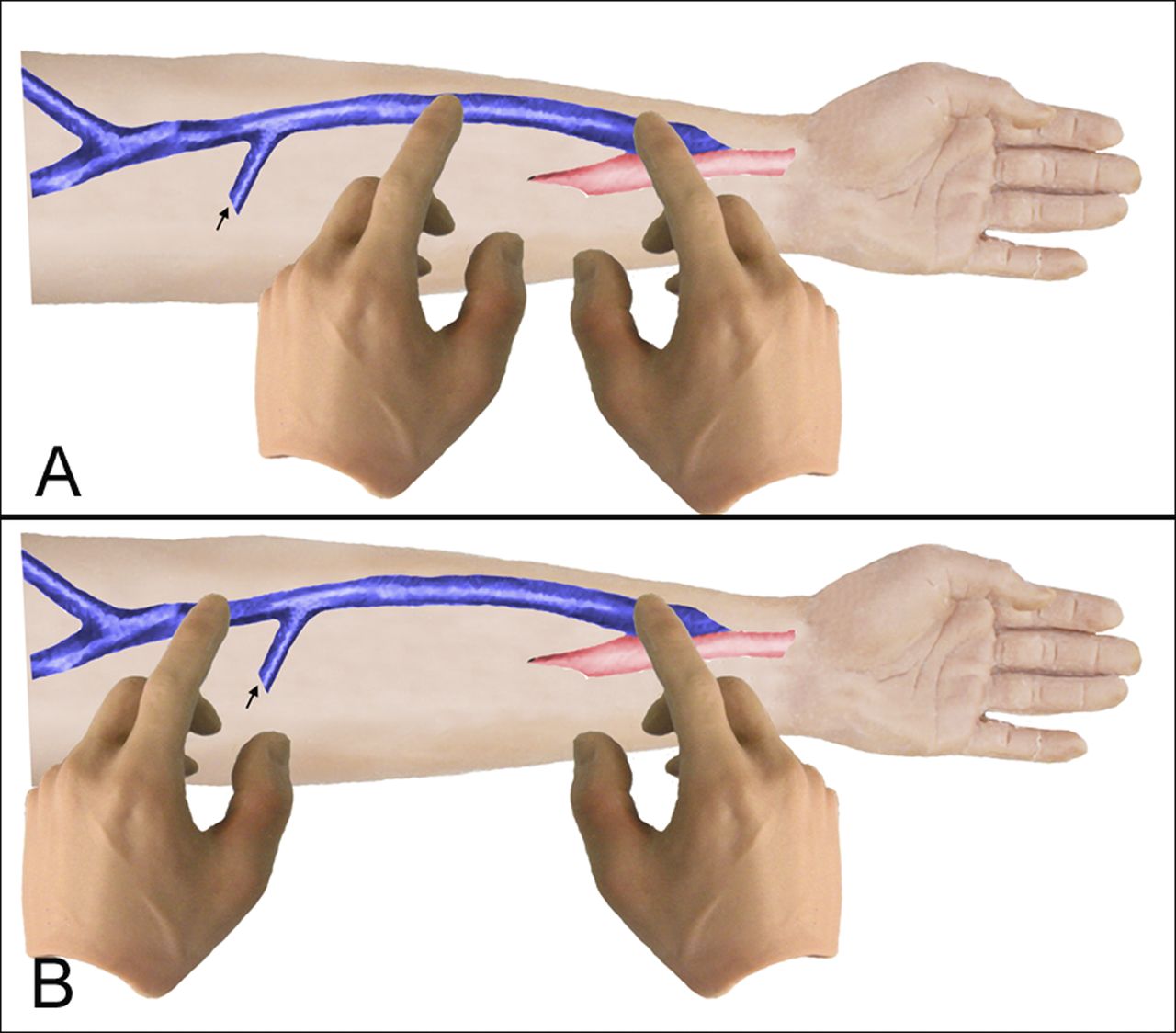
Figure 12. The sequential occlusion test. The left hand (occluding hand) gradually moves farther from the right hand (palpating hand), assessing the pulse each time the access is occluded. If the access is occluded distal to a collateral vein, the thrill will stop and the pulse will intensify (A). If the access is occluded proximal to the collateral vein, the thrill will continue and no pulsation will be felt (B). From Salman and Beathard, CJASN, 2013
| Clinical Pearl: An absent bruit and/or thrill is concerning for AV access thrombosis. Patients should be referred to an interventionalist or surgeon for urgent thrombectomy (“declot”) as soon as thrombosis is suspected. Consider cardiac evaluation, as low LVEF may be a cause for recurrent thrombosis. |
Auscultation (Listen)
A stethoscope should be used to listen along the entire length of the AV access. A normal bruit should sound like a continuous (systolic and diastolic) hum. The normally low-pitched bruit will become squeaky and high-pitched if hemodynamically significant stenosis is present. As with the thrill, a stenotic lesion will cause the bruit to lose its diastolic component.
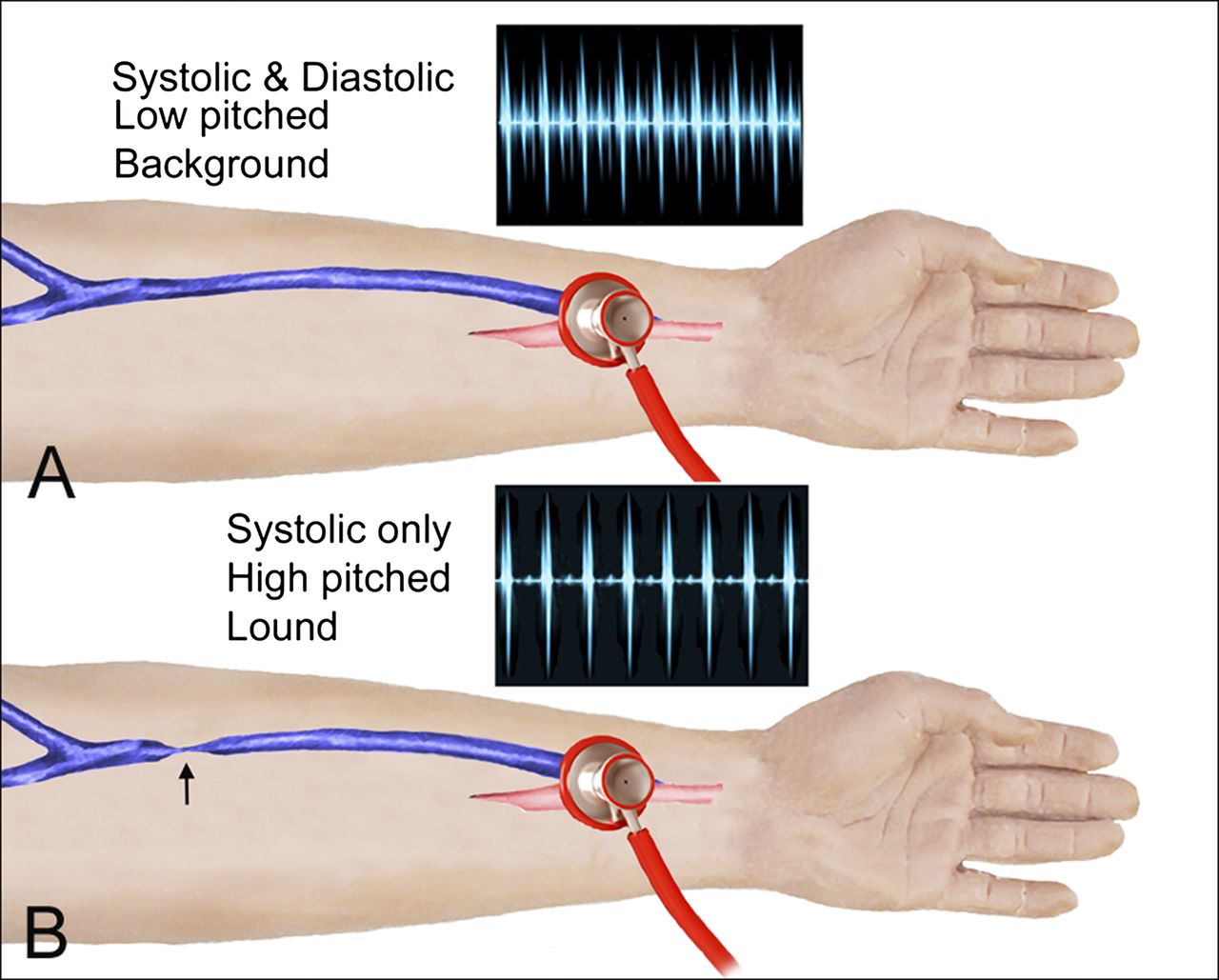
Figure 13. Auscultation of an AV access. From Salman and Beathard, CJASN, 2013.
SummaryPhysical examination of hemodialysis vascular access is an important skill for all nephrologists to have. Any abnormal findings should prompt referral to an interventionalist for further evaluation. Learning how to conduct an AV access examination can have significant impact on patient care
Your Turn!
Practice your vascular access diagnostic skills with the following cases from NephSim:
Post by: Crystal Farrington, ASDIN Fellow
Acknowledgments: This post is part of a collaboration between the Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. Special thanks to Tushar Vachharajani, Aisha Shaikh, Edgar Lerma, and the Education Committee of ASDIN for their comments and suggestions for this post. For more information about the ASDIN mission or membership, click here.

Is High out flow fistula will collapsed on arm elevation???
Thank you ! Very nice.
Great summary of the vascular access’ physical examination. Keep up the good work.
Nice
Fistula is best vascular acssess..
Decrease risk of infection.
Crisp and precise, thanks !!!
This is a great tool, it took me a long time during my neph fellowship to get comfortable with HD access examination. This is really helpful.
I like this
I recommend that to added this to the book of physical examination.
Thanks
Excellent 🤗 way about examination of vascular access
Nice