Our review of normal kidney histology concludes with the vasculature. The kidneys are richly vascular organs, receiving approximately one-quarter of the cardiac output. The renal vascular architecture is unique and complex, allowing the kidney to perform its many physiological functions. These features also have several implications for disease processes affecting the kidney.
Vascular Architecture
The blood supply to the kidneys originates from the paired renal arteries, which branch into segmental arteriesat the renal hilum. The segmental arteries divide into interlobar arteries, which penetrate the renal capsule and travel up through the renal columns between renal pyramids. The interlobar arteries branch into arcuate arterieswhich run along the corticomedullary junction. From the arcuate arteries radiate the interlobular arterieswhich extend up into the cortex and finally become the afferent arteriolesof glomeruli. After filtration occurs, the glomerular capillariesconverge into the efferent arterioles, which give rise to either the peritubular capillariesor the vasa rectadepending on the location/depth of the glomerulus. The venous systemdrains the kidneys in a similar distribution as the arteries. Our discussion will focus on the arteries, arterioles, and specialized capillary beds.
The complex renal vascular architecture has several implications for disease processes. First, given the segmental nature of the renal blood supply and the lack of significant collateral circulation between segments, occlusion of a branch usually results in ischemia and infarction of the area it supplies (the arteries are functional end-arteries). Second, all of the tubular capillary beds are derived from the efferent arterioles. Therefore, if the blood flow of a glomerulus is affected by a disease process, so is the blood flow to the tubules (the entire nephron is affected). Also, the blood supply of the medulla is derived from glomerular efferent arterioles. As the medulla is already at very low levels of oxygenation, it is very sensitive to changes in blood oxygenation.
Arteries
The arteries most commonly encountered on kidney biopsy are the interlobular arteries of the cortex, followed by the arcuate arteries at the corticomedullary junction. All arteries are muscular arteries with an intima, muscularis, and adventitia.
The larger arteries (main renal, interlobar, and arcuate) have both an internal and external elastic lamina on either side of the muscularis, which typically contains more than 5 layers of smooth muscle cells. The smaller (interlobular) arteries only have an internal elastic lamina, and usually contain 3-5 layers of smooth muscle cells in the muscularis. In normal arteries, there is no discernable space between the endothelial cells and internal elastic lamina. With aging and in many pathologic conditions including hypertension, there is thickening of the intima by deposition of connective tissue (fibrosis) and replication of the internal elastic lamina.

Arterioles
Arterioles are easily identifiable throughout the renal parenchyma. Afferent and efferent arterioles can be seen entering and exiting glomeruli at the vascular poles. Arterioles have no identifiable internal or external elastic lamina, and typically contain 1-2 layers of smooth muscle cells in the media. In pathologic conditions including hypertension and diabetes, insudation of plasma proteins can be seen expanding the arteriolar walls in the form of amorphous, PAS-positive hyaline.

Capillaries
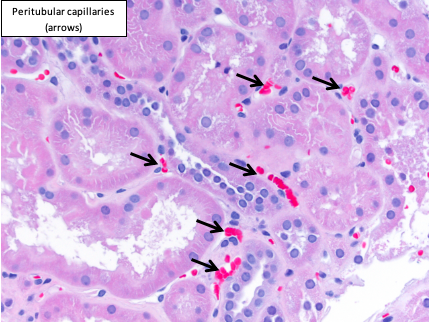
The afferent arteriole branches into glomerular capillaries immediately after entering the glomerulus. The cortical peritubular capillaries derive from the efferent arterioles of the superficial cortical glomeruli.
Peritubular capillaries appear as “spaces” between the tubules, which may contain occasional circulating red or white blood cells. They are composed of a single layer of endothelial cells invested by basement membrane and pericytes. The most common pathologic change seen in the peritubular capillaries is leukocytic infiltration (termed “peritubular capillaritis”), which is particularly important in the transplant setting.

Vasa Recta
The vasa recta, or “straight vessels,” derive from the efferent arterioles of the deeper (juxtamedullary) glomeruli. The vasa recta are capillaries that loop down into the medulla to form a plexus around the medullary nephron segments, particularly the loops of Henle. Descending and ascending vasa recta are grouped into vascular bundles.

Kammi J. Henriksen, MD
Assistant Professor of Pathology, University of Chicago

