More than 30-million Americans are living with diabetes and 90% of these people have type 2 diabetes mellitus (DM2). There are numerous complications associated with long-term diagnosis of DM2, with a prominent concern being the development of impaired kidney function. In fact, diabetes is the most common cause of end-stage kidney disease (ESKD) and despite decades of research working to better understand this relationship, there have been limited treatment options available to slow the progression of kidney disease in people with DM2.
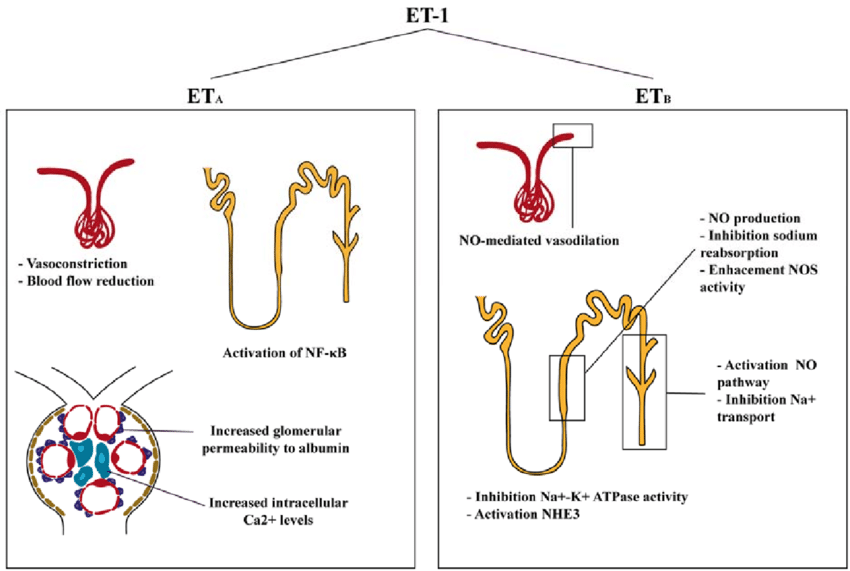
The endothelin (ET) system plays an important role in the development of diabetic nephropathy. The ETA receptors are largely responsible for the vasoconstrictive and proliferative actions of the potent peptide ET-1. David Pollock and colleagues have probed extensively at the mechanism in which ETA receptors contribute to the diabetic kidney disease. They’ve demonstrated that ET-1, via the ETA receptor, directly increases the glomerular permeability to albumin, nephron loss, and increases inflammation. In this line, using diabetic kidney disease models, selective blockade of the ETA receptor reduced proteinuria, glomerular permeability, restored glomerular filtration, and had anti-inflammatory and antifibrotic effects. Findings from this study and others have provided evidence and support for the use of selective ETA antagonists as a treatment for diabetic kidney disease.
Many Phase 3 clinical trials have been conducted over the past decade, however most have failed to be effective or had side effects that precluded their use. Even so, there is substantial evidence supporting that endothelin receptor antagonists (ERAs) could be a therapeutic approach to diminish the burden of kidney disease in people with DM2. A previous clinical trial, the ASCEND trial, helped set the stage for ERAs. The ASCEND Study Group investigated if treatment with Avosentatn, an ERA, would protect from progressive loss of renal function in people with DM2. While they observed reduced albumin-to-creatinine ratio, the study was terminated after 4-months due to an excess of cardiovascular events, mainly fluid overload and congestive heart failure. However, since the ASCEND trial, newer and more specific ERAs have been designed and a new trial has emerged, the SONAR trial: the Study Of diabetic Nephropathy with AtRasentan.
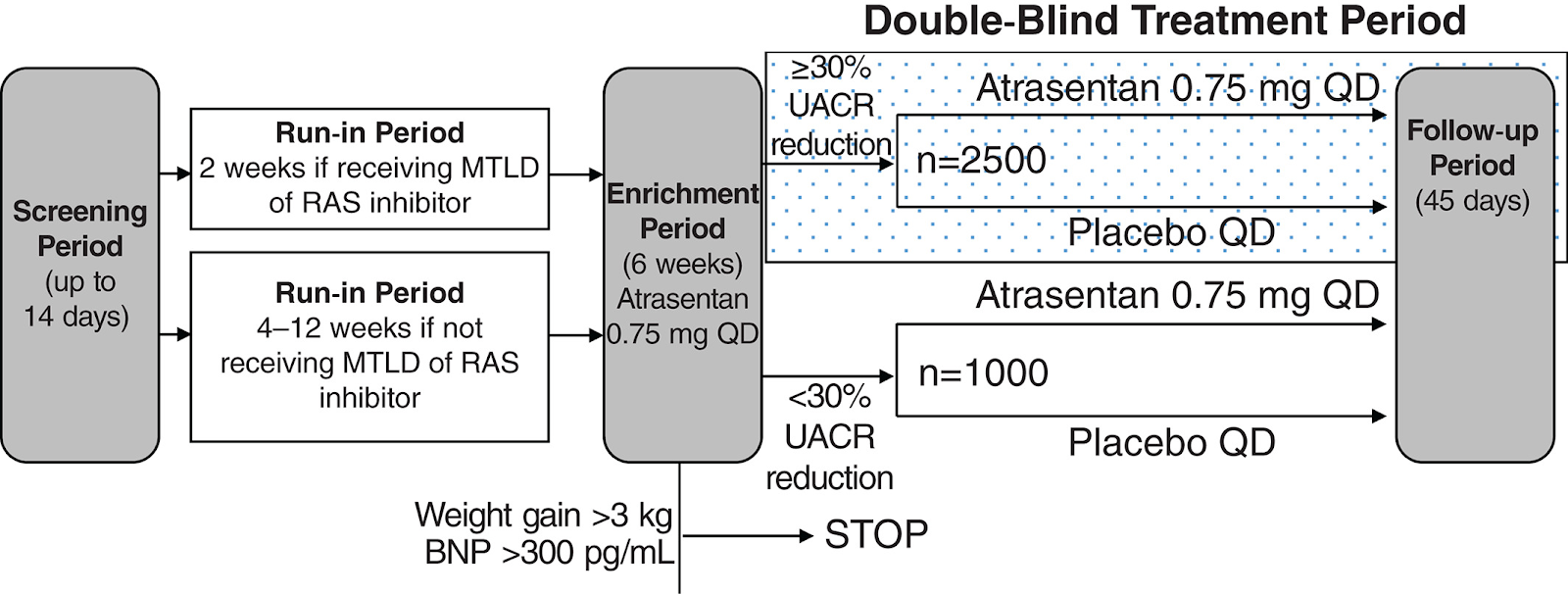
The SONAR trial is a Phase 3 Clinical trial that utilized a double-blind placebo controlled study design to investigate the efficacy of atrasentan in delaying the progression of kidney disease in people with DM2. Atrasentan is an ETA antagonist that has demonstrated the ability to decrease albuminuria in patients with diabetes when taken in conjunction with a maximum tolerated dose of an angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB).
During the trial, 2648 patients were included as responders and 6% (79) of the 1325 patients in the atrasentan group had a primary composite renal endpoint event compared to 7.9% (105) of the 1323 patients in the placebo group (95% CI 0.49-0.88; p=0.0047). The atrasentan group experienced greater fluid retention, as listed as an adverse event, but experienced fewer heart failure hospital admission than the placebo group. The overall conclusions from the study supported the potential role of atrasentan in protecting renal function in people with DM2 at high risk of developing ESKD.
Perhaps the most interesting aspect of the SONAR trial is their different and unique study design compared to other clinical trials. This study utilized a response enrichment design. This design strategy only includes patients who are more likely to show benefit or enrichment of the treatment based on a >30% reduced UACR during a 6-week open label enrollment period. Therefore, the trial is only including patients who are likely to benefit and excluding those who are unlikely. The use of an enrichment design is an interesting approach to clinical trials, and certainly one can see the good and the bad to this design.
On one side, the use of an enrichment design is a potential way to make drug development more successful and efficient. As previously mentioned, previous clinical trials, like BEACON, ASCEND, or RADAR, using similar therapeutic targets were terminated early due to adverse events. In fact, this is the case for many clinical trials across all fields and the success rate of a drug passing Phase III of clinical trials is only 25-30%. However, these studies are large scale and include any persons with the disease or condition. Knowing that each drug could affect individuals differently and have various efficacy, is this gunshot strategy the always best approach in determining if a drug move to market or not?
While large scale testing, as done in Phase III trials, is very much necessary to identify all potential adverse outcomes, it can often lead to early termination of potentially beneficial therapies for a subpopulation of individuals. The enrichment design used in SONAR expanded on previous trials using atrasentan but focused on patients who were most likely to benefit from the treatment. The patients that were positively benefiting with minimal or managable side-effects were able to continue to improve in health while those who were not, no longer were put at risk with the treatment.
On the flip side of this debate, an enrichment design is an attempt to ensure the positive outcome results. It eliminated patients most likely to experience the expected adverse outcomes (i.e. volume overload) and while I believe it is incredibly important to explore and identify all beneficial therapy options, is this window too small for the pharmaceutical industry? How would we translate this to the clinic and determine who are the responders or who will have the adverse outcomes early on and before the treatment is given?
The SONAR trial design has certainly raised some interesting questions and overall, has introduced an attention-grabbing approach for clinical trials in not only diabetic kidney disease, but other clinical trials focused on high risk populations. The recent results also expanded on the exciting therapeutic benefit of atrasentan on renal outcomes in progressive renal dysfunction and cardiovascular events in people with DM2.
Casey Derella
PhD Student at Augusta University

