Currently, the timing of initiation of renal replacement therapy (RRT) in critically ill patients with acute kidney injury (AKI) remains a challenge. T Despite several randomized controlled trials (RCTs) comparing early versus late initiation strategies of RRT, the results are ambiguous. Let’s review some of landmark studies in this area.
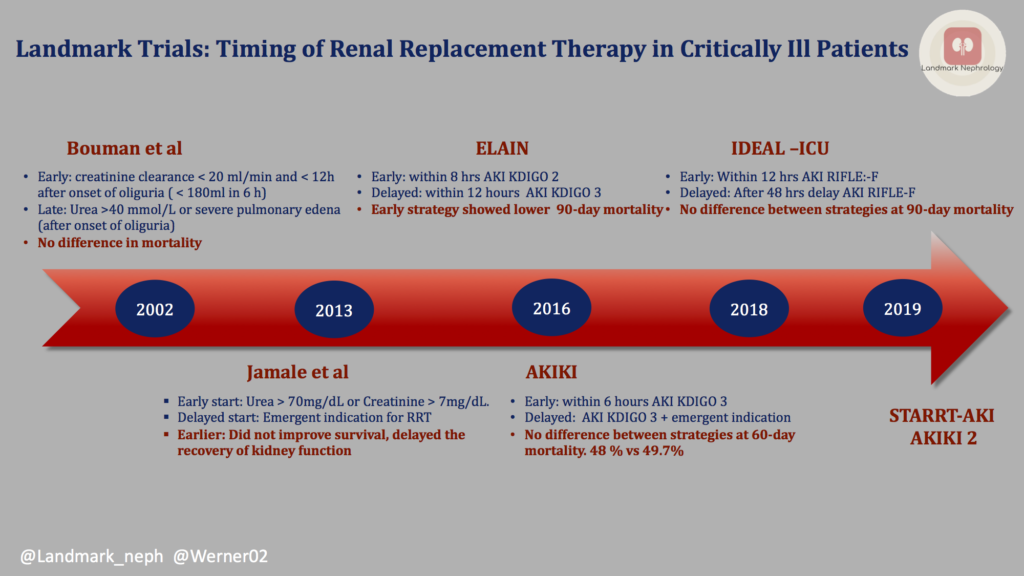
First, let’s examine the data that have led up to the modern day trials of ELAIN, AKIKI, and IDEAL-ICU. In the table below, we summarize 3 important RCTs from 2002 – 2013.
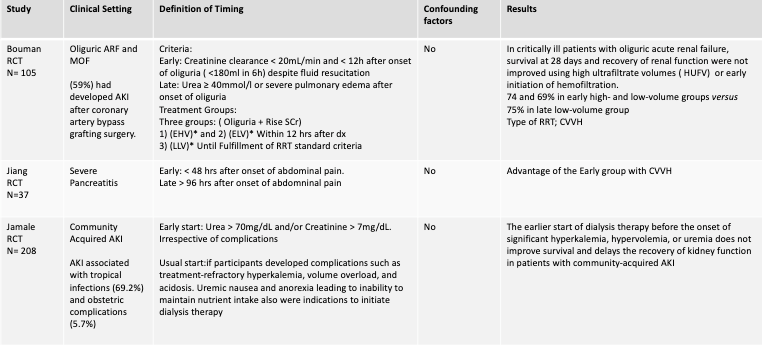
Though some retrospective studies favored “early” start of RRT, the RCTs above did not show any clear benefit. Importantly, the definition of “early” vs “late” was heterogeneous among these small studies. We’ll now review the more recent RCTs: ELAIN, AKIKI, and IDEAL-ICU.
1. ELAIN
In 2016, Zarbock et al in Germany evaluated the effect of Early vs. Delayed initiation of RRT on mortality in critically ill patients with AKI. 93.5% of patients had AKI after surgery, of which 46.75% were cardiac surgery patients. This study demonstrated a significant reduction in 90-day mortality with the EARLY strategy (AKI KDIGO 2), in a group of almost entirely surgical patients.
Patients were divided into two groups for the initiation of RRT:
- EARLY: Within 8 hours with AKI KDIGO stage 2 and a Neutrophil Gelatinase-Associated Lipocalin (NGAL) > 150 ng/ml.
- LATE: Within 12 hours of either AKI KDIGO stage 3 or an absolute indication for RRT.
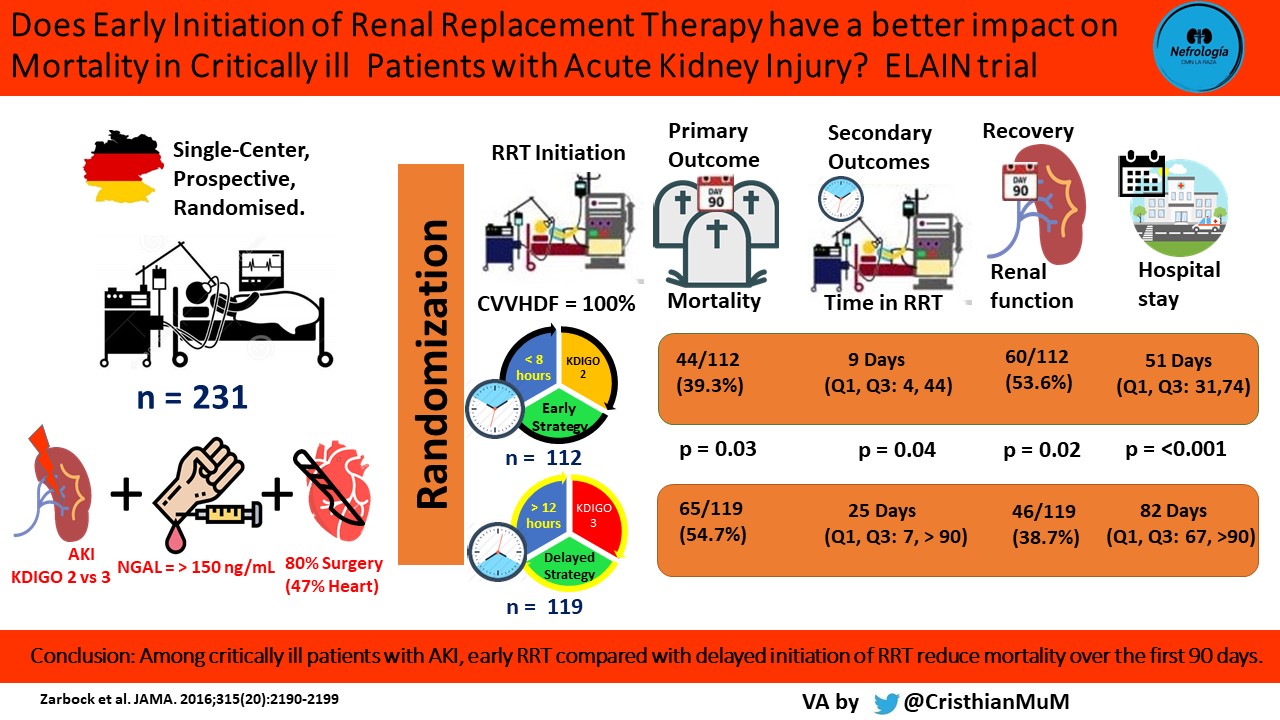
Nearly 75% of patients (in both groups) developed fluid overload, 88% of needed catecholamines >0.1 µg/kg/min prior to initiation of RRT, and the first-line RRT modality was continuous venovenous hemodiafiltration (CVVHDF).
Weakness of this study: first, it had a Fragility Index of 3 – meaning that a shift of only 3 patients from the event to non-event group would render the findings statistically insignificant. ELAIN was a single center study in Europe and not all the treatments were standardized between groups. Treatments were unblinded by the nature of starting the treatment, possibly introducing bias and challenging its internal validity.
2. AKIKI
Also in 2016, Gaudry et al published the AKIKI trial. They defined early versus delayed RRT as:
- EARLY: within 6 hours from randomization with AKI KDIGO stage 3.
- DELAYED: RRT was initiated if the patient developed AKI KDIGO 3 plus dialytic emergency
The choice of modality, duration, and interval between sessions of RRT was left to the discretion of each study site and was prescribed and monitored according to national guidelines. As a result, over 50% received intermittent RRT.
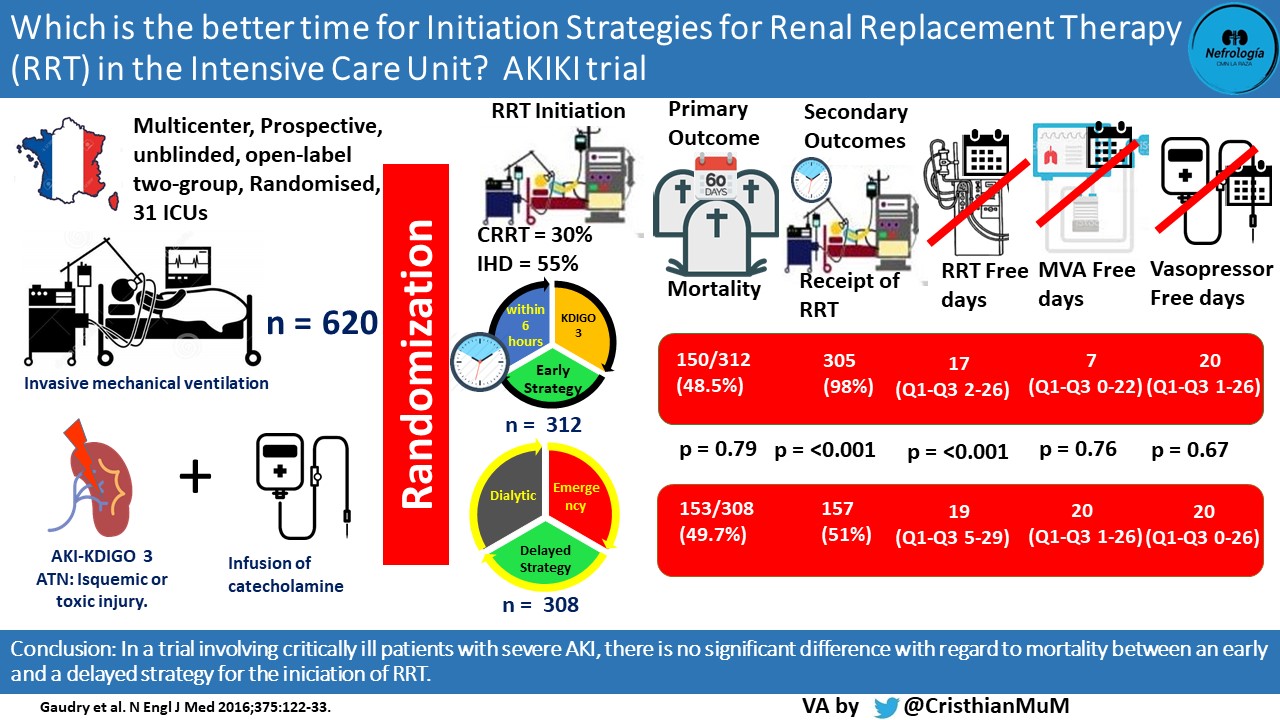
AKIKI had more critically ill patients with severe AKI than the ELAIN trial. Unlike the ELAIN study, the main reason for ICU admission was a medical rather than surgical indication (~66% septic shock in both groups, 20% surgical cases). The primary outcome showed no significant difference in mortality between early strategy and delayed strategy of RRT. Over 50% of patients received the initial modality of intermittent hemodialysis (HD), despite the fact that 85% of patients required vasopressor support upon initiation of RRT.
Weakness of this study: A major weakness was that it only included patients with advanced kidney injury, and therefore the results may not be generalizable to patients with less severe AKI. This trial, like ELAIN, was not blinded by the nature of the treatment.
The results between ELAIN and AKIKI were divergent with key differences, and they did not fully answer the question of the ideal timing of RRT initiation. Two years later in 2018, Barbar and colleagues published the IDEAL-ICU trial. This RCT importantly included more patients with sepsis than ELAIN and AKIKI which is clinically relevant as it is the number one cause of AKI in hospitalized patients.
The authors defined early versus delayed initiation of RRT as:
- EARLY: RRT was started within 12 hours after the onset of AKI RIFLE Stage F.
- DELAYED: RRT was initiated after a delay of 48 hours of AKI RIFLE Stage F
The choice of RRT technique (intermittent or continuous) was at the discretion of clinical experts at each site.

Continuous slow therapy was used as initial modality in 57% of the patients assigned to the early strategy group, and in 55% of those in the delayed group (p = 0.62).
In the delayed strategy group, 29% of the patients did not require RRT because they had spontaneous recovery of renal function. This lead to a difference in actual receipt of RRT with 97% in early group vs. 62% in the delayed group (p=0.001). Nonetheless, 17% (41 patients) of the late strategy group developed an absolute criterion for the initiation of RRT before reaching 48-hours after the diagnosis of AKI in stage F. The mortality of these patients was 68%, higher than the general mortality (55%).
This trial showed no statistically significant different in the primary outcome (mortality) between early versus late initiation of RRT patients with septic shock and severe AKI.
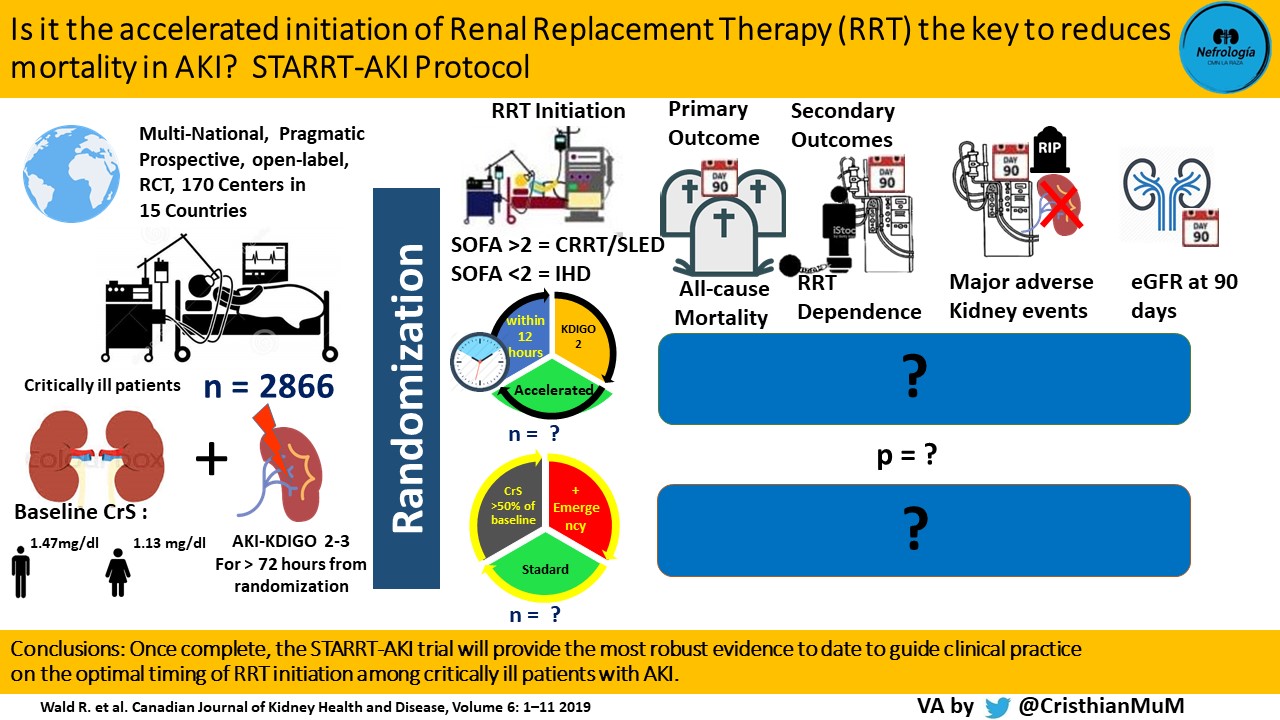
4. STARRT-AKI & AKIKI 2: Ongoing…
The study protocol for the ongoing STARRT-AKI trial is outlined below. The investigators reported this month that they have enrolled their entire cohort.
The AKIKI 2 trial is also underway. which will also compare early versus late initiation of RRT in patients with AKI.
Conclusions:
Completed RCTs thus far have not provided consistent evidence for the early initiation of RRT in critically ill patients with AKI, though there may be some benefit in post-operative patients who undergo cardiac surgery. The comparison between each RCT is challenging, due to different causes of acute kidney injury in their populations as well as definition of AKI and “early” versus “late” initiation of RRT.
More to come on this topic, stay tuned…
Post by:
Cristhian Muñoz Menjivar
A.Verner Venegas Vera
Hugo Cesar Campos Gil
Gates B Colbert
i hope a centre i Africa could share in such multicentre studies, it will be additive giving the large number of AKI in ICU patients.
You’re welcome Brenda, We are glad to help
Thanks for this.