We can expect standardized exams to contain some of the same questions every year. Certain disorders have pathophysiology that seamlessly transitions from basic science to clinical presentation. Others have such striking radiographic imaging that they inevitably end up on a vignette. As such, their prevalence on exams is much higher than that observed in real life. Below is a collection of visual mnemonics that will hopefully make some of these questions easier on your next test.
Gordon Syndrome
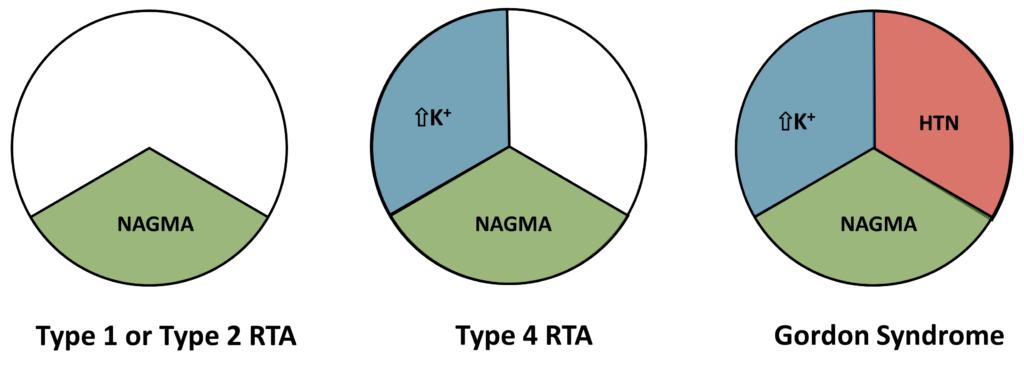
Several disorders on board exams can cause non anion gap metabolic acidosis (NAGMA). Pseudohypoaldosteronism type 2, aka Gordon Syndrome, has a phenotype that includes NAGMA, hyperkalemia, and hypertension (HTN). It is caused by with no lysine (WNK)4 or WNK1 mutations or even mutations affecting the proteins that degrade WNK4 or WNK1. Various types of renal tubular acidosis (RTA) should be kept on the differential diagnosis, but have a slightly different presentation.
Hypertensive Disorders Associated with Intracranial Aneurysms
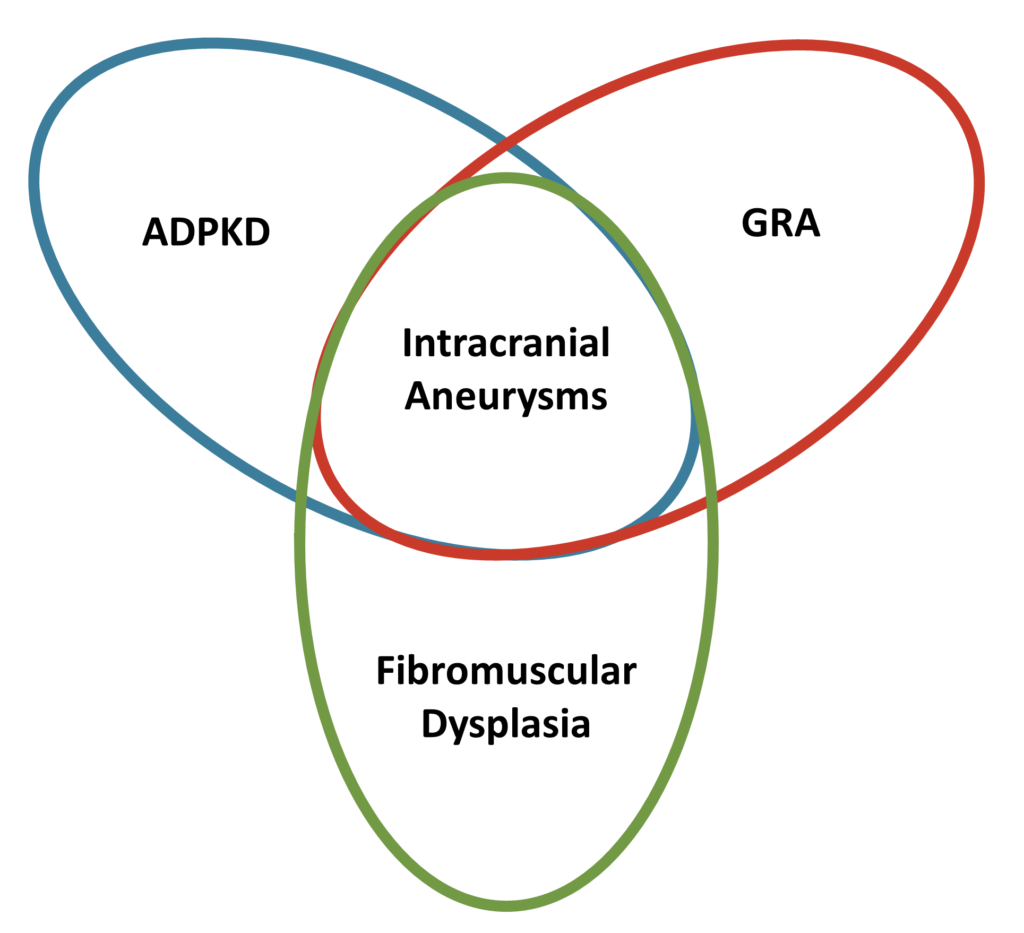
Several disorders are associated with both hypertension and intracranial aneurysms. Autosomal dominant polycystic kidney disease (ADPKD), glucocorticoid-remediable aldosteronism (GRA), and fibromuscular dysplasia are the three that could end up on exams.
Geller Syndrome

Activating mineralocorticoid receptor mutation (Geller Syndrome) is a polar opposite of primary aldosteronism in some respects. Although both primary aldosteronism and Geller Syndrome present with HTN, hypokalemia, and metabolic alkalosis, they differ in their response to pregnancy and spironolactone. For the board exam, watch for a patient presenting with worsening hypertension, hypokalemia, and normal aldosterone levels during pregnancy. Additionally, spironolactone actually raises blood pressure in Geller Syndrome patients. Therefore, spironolactone should not be used for BP control in Geller Syndrome patients.
Angiogram Pictures of the Kidney

There are essentially only three reasons you would see an angiogram of a kidney on a test. Atherosclerotic renal artery stenosis and fibromuscular dysplasia cause hypertension, but present in different patient populations. Atherosclerotic renal artery stenosis is most often seen in older adults with coronary artery disease or similar risk factors. Fibromuscular dysplasia is seen in younger females with few or no risk factors for coronary artery disease. Polyarteritis nodosa is a vasculitis that affects medium-sized arteries. On test questions, it will present with fever, arthralgias, skin lesions, neuropathy, gastrointestinal symptoms, hypertension, reduced kidney function, and renal arterial aneurysms as shown on the picture.
Elevated Osmolal Gap
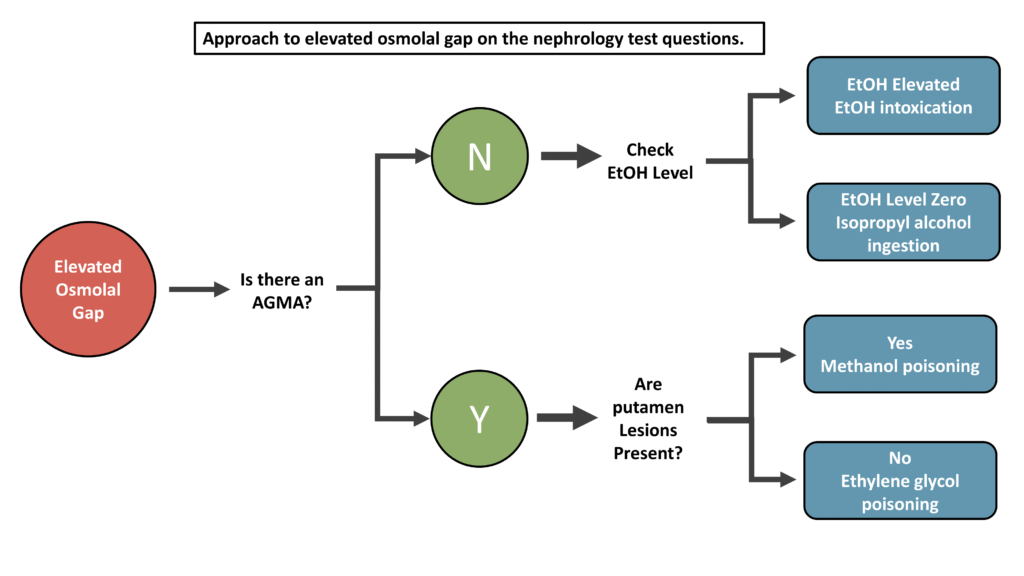
You will absolutely get test questions on anion gap metabolic acidosis (AGMA) and elevated osmolal gaps. The mix of answer choices for questions involving these types of disorders are variable, but the algorithm above simple way to approach vignettes involving an elevated osmolal gap.
Genetic Kidney Syndromes
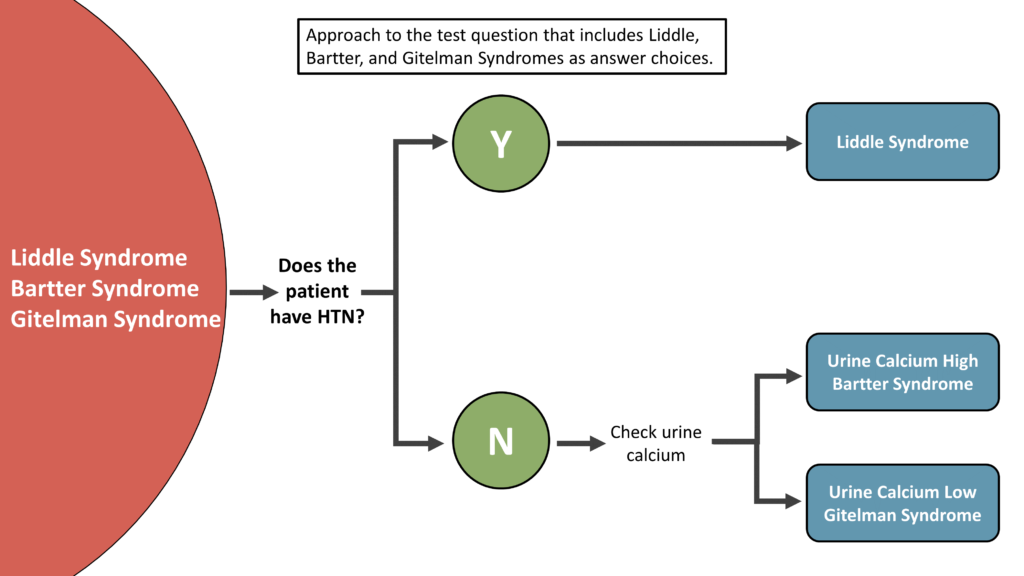
You will inevitably face a question with Liddle, Bartter, and Gitelman Syndromes as answer choices. Initially this is an intimidating question, but by looking at the blood pressure and urinary calcium excretion, you can quickly arrive at the proper diagnosis. Always remember — Bartter Syndrome acts like a loop diuretic and Gitelman Syndrome acts like a thiazide diuretic.
Gerren Hobby, MD
Nephrologist
Arkansas
NSMC Intern 2020
@ghobby

Appreciate. Wonderful
These are some great visual tips for studying! Comparison tables, flowcharts & summaries require some time investment to make, but we tend to underestimate the long lasting memories they produce vs simple re-reading. Thank you for writing this article!
Very helpful and precise and concise. Great job.