Elevated intracranial pressure (ICP) is a neurologic emergency that is associated with poor outcomes. It may be caused by traumatic brain injury, intracerebral infarction or hemorrhage, subarachnoid hemorrhage, and CNS tumors.
Mannitol has long been the first-line osmotic therapy in the medical management of elevated ICP. Its mechanism of action is classically attributed to its ability to reduce brain volume by exerting osmotic effects– drawing free water out of brain tissue into the circulation and eventually excreted by the kidneys. However, its many adverse effects such as volume depletion, electrolyte abnormalities and acute kidney injury (AKI) from mannitol toxicity have limited its use.
Because of this, the use of hypertonic saline solution (HSS) as an osmotic agent is now becoming more frequent.
Hypertonic Saline: Good or Bad for Patients with Elevated Intracranial Pressure?
The Good
Studies on the use of hypertonic saline to reduce brain swelling have gone as far back as the 1920s, when an American neurosurgeon, Dr. Harvey Cushing (of Cushing’s triad), and a urologist named Dr. Frederick Foley (designer of the Foley Catheter) described the use of oral hypertonic saline, first in a cat, and then in patients with brain tumors and subsequent brain herniation after decompressive surgery. The study was exploratory, but they found it to be effective in lowering tension and described “very striking results could be obtained in which case the tense convex protrusion became a soft concave area over the decompression site”.
Similar to mannitol, the main mechanism behind HSS is attributed to its ability to create an osmotic gradient across the blood brain barrier, thereby leading to a reduction in brain water content, decreased intracranial pressure and prevention of further injury. Its theoretic benefit over mannitol is due to the higher reflection coefficient of sodium (=1) making it less permeable across the blood brain barrier, and more effective in pulling water out of the tissue and interstitial space without any theoretical rebound.
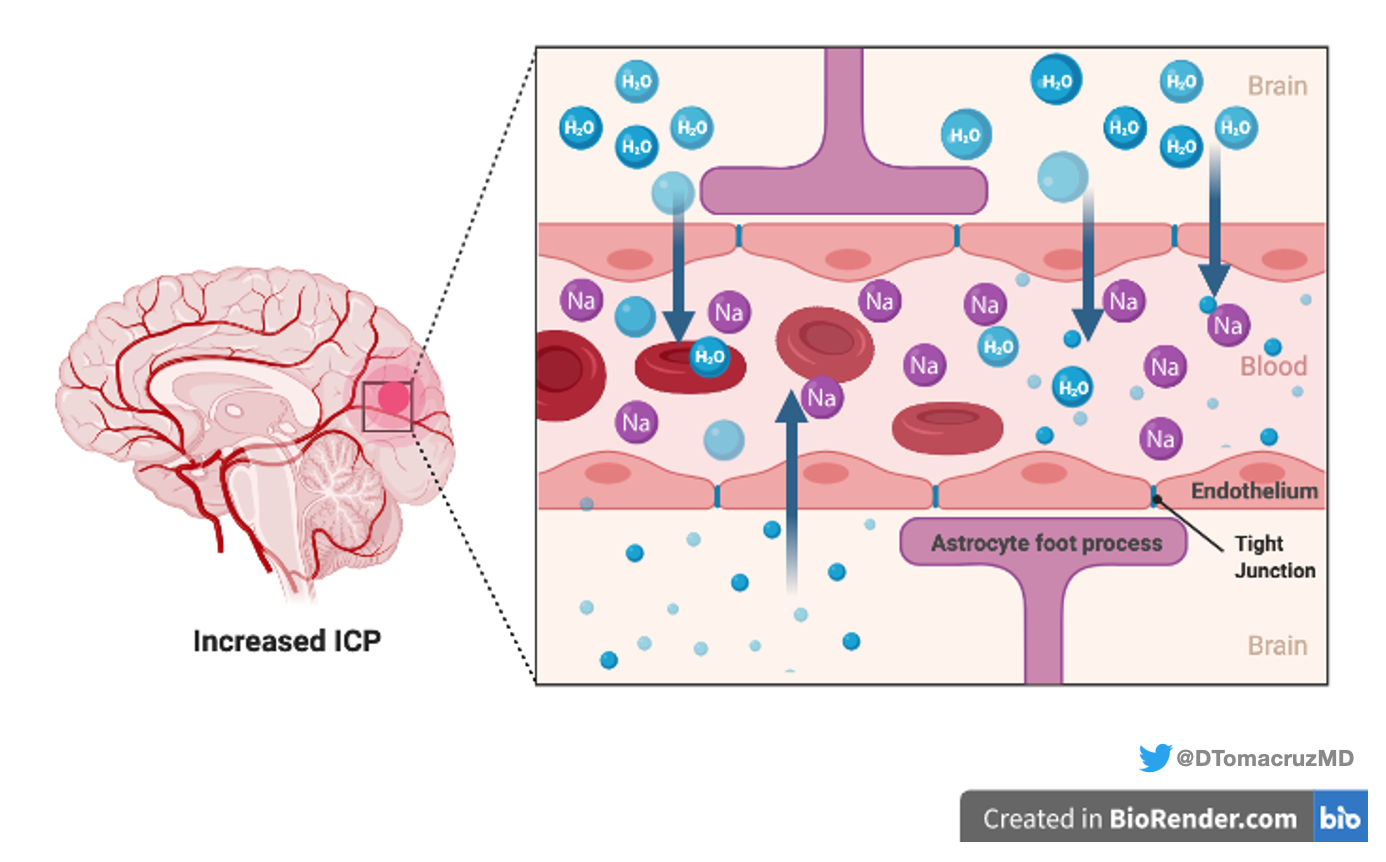
HSS exerts its hemodynamic activity by acting as a plasma volume expander, thereby improving blood pressure, increasing cardiac output and cerebral perfusion pressure.
Other immunomodulatory and hemodynamic mechanisms have also been proposed, some of which include better cerebral blood flow from reduced blood viscosity, autoregulatory vasoconstriction, and endothelial cell shrinkage with subsequent microcirculatory improvement.
Several randomized controlled trials conducted decades later, have compared HSS with mannitol in different clinical scenarios of increased ICP. Two recent meta-analyses by Kamel et al and Mortazavi et al suggested HSS to be equally if not more effective than mannitol in decreasing ICP. However, outcomes on mortality have not been clearly established and the data was limited by the small number of RCTs, low patient numbers, and inconsistent methods between studies. Larger, multicenter RCTs are still lacking.
The (Possibly) Bad
Some may agree that the use of HSS among neurologists has increased steadily over the years and referrals to nephrologists have become more frequent due to problems encountered such as hyperchloremia and AKI.
Three studies published in 2017 have explored the incidence of hyperchloremia and AKI among neurocritically ill patients (Table 1). The study by Riha et al found that patients with hyperchloremia had a higher risk of AKI and in-hospital mortality even after adjusting for differences among patient groups. The second study by Erdman et al found a 16% prevalence of AKI by AKIN criteria, among patients using continuous infusion of HSS with or without mannitol. Hyperchloremia was also more common in the AKI group compared to the non-AKI group (80% vs 55%). The study by Sadan et al primarily evaluated the prevalence of AKI by KDIGO, among patients with subarachnoid hemorrhage (16.7%); however, they later found that patients who developed AKI received more HSS and, in fact, identified HSS and mean serum chloride concentration to be some of the predictors of AKI. There are several limitations in these studies. Patients with AKI were sicker— with more depressed sensorium, higher intracerebral hemorrhage scores, longer durations of mechanical ventilation and longer lengths of ICU stay. This makes it difficult to draw definite conclusions if the incidence of mortality or AKI was due to hyperchloremia alone, or due to other confounding factors.
Table 1. Studies on Hyperchloremia and AKI among Neurocritically Ill Patients
| Study | Patient Population | Study Groups | Outcomes |
| Riha et al., 2017 Multicenter, retrospective, propensity matched cohort | Patients with intracerebral hemorrhage receiving 3% HSS (continuous infusion) (n= 219) | Moderate Hyperchloremia (Cl>115)(n=143)vs Nonhyperchloremia (n= 76) | In-hospital mortality:Moderate Hyperchloremia 34% vs Nonhyperchloremia 14% (p=0.02) Moderate hyperchloremia independently predicted in-hospital mortality (OR 4.4) [95% CI, 1.4-13.5] (p = 0.01) |
| Erdman et al., 2017 Multicenter, retrospective cohort | Neurocritical patients receiving HSS (continuous infusion +/- mannitol, or HSS boluses) (n= 329) | AKI(n=54)VsNon-AKI(n=283) | Prevalence of AKI by AKIN criteria (16%) Hyperchloremia (>110mmol/L):AKI 79.6%Vsnon-AKI55.1%(p<0.01) MortalityAKI (48.1%) vs non-AKI (21.9%)p<0.001 |
| Sadan et al., 2017 Retrospective analysis | Patients with subarachnoid hemorrhage (n=1267) | AKI (n=212)vsNon-AKI(n=1055) | Prevalence of AKI by KDIGO (16.7%) Increase in mean serum chloride concentration (per 10mmol/L) was associated with development of AKI:(OR 7.39)(95% CI 3.44-18.23) Mortality AKI (28.3%)Vsnon-AKI (6.1%)(p<0.01) |
Why bother with chloride?
Studies on the deleterious effects of supraphysiologic chloride concentrations in intravenous fluids sound all too familiar. The use of normal saline has long been the intravenous fluid of choice among several physicians; however newer studies demonstrating adverse events of hyperchloremia have led us to question its impact particularly on the kidneys.
Chloride is the main extracellular anion and plays a major role in acid-base balance. It is a Stewart strong ion that exists mainly in a dissociated state, thereby exerting effects on blood pH. The normal plasma concentration of chloride is ~ 100mmol/L. Administration of fluids such as normal saline (and more so HSS, with a chloride concentration ranging from 500-1300 mmol/L ) causes a significant rise in chloride concentration and notable drop in pH. But the effects of chloride seem to extend beyond its effect on acid base balance.
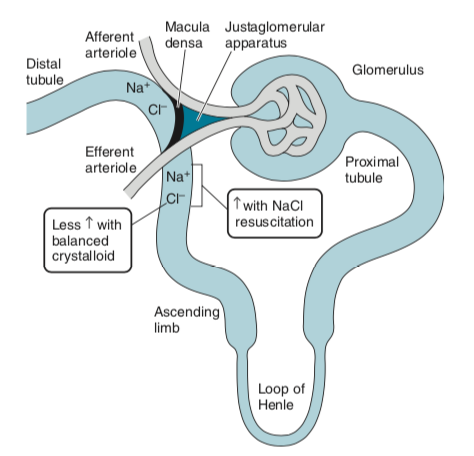
It is said that increased chloride delivery in the kidneys may result in:
(1) arteriolar vasoconstriction via the tubuloglomerular feedback
(2) thromboxane release increasing both afferent and efferent arteriolar resistance, as well as
(3) drops in mean arterial pressure– which all lead to decreased renal perfusion, reduction in GFR and acute kidney injury
Do you remember the SMART and SALT-ED trials? More on chloride and its deleterious effects on the kidneys are explained in the 2018 NephMadness Hospitalist Nephrology Region.
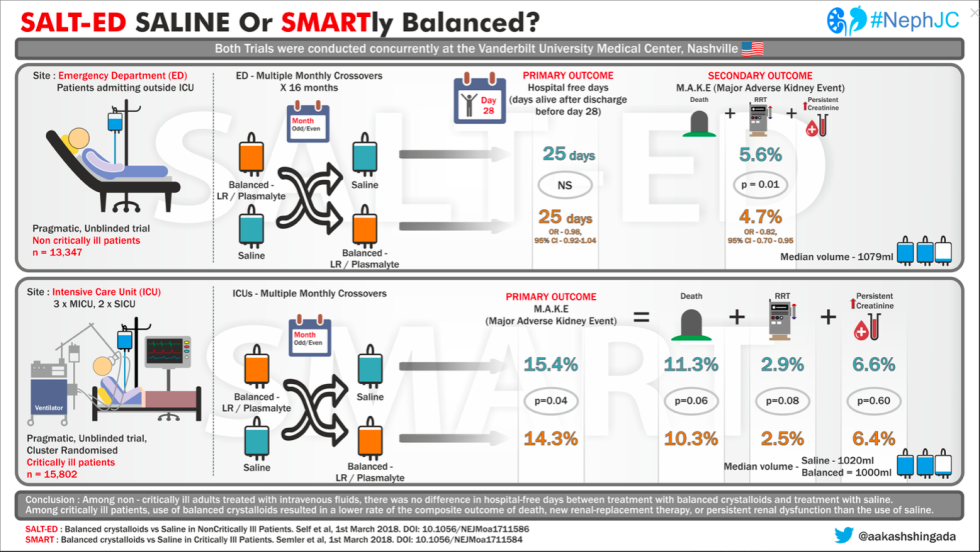
These recent trials demonstrate that although the amount of fluids administered was relatively small, the use of balanced crystalloids resulted in a lower incidence of major adverse kidney events (defined by a composite of death, new kidney replacement therapy, or persistent kidney dysfunction).
Now going back to HSS…
Chloride content in some common formulations of HSS used in the neurologic setting
Some of the HSS preparations available include:
| Sodium Chloride | Typical Initial Bolus (mL) | Osmolarity (mOSm/L) | Na concentration (mEq/L) | Cl concentration (meq/L) |
| 3% | 150-250 | 1026 | 513 | 513 |
| 7.5% | 100-150 | 2566 | 1283 | 1283 |
| 23.4% | 30 | 8008 | 4004 | 4004 |
Protocols on its use vary per institution. Some give it in boluses, others use continuous infusion with a central line.
Monitoring
To achieve the desired osmotic gradient and reduce ICP, most protocols use the approach of targeting a level of serum sodium of 145-155 mmol/L. Careful monitoring of serum sodium levels every 4-6 hours is done to avoid overshooting these levels. It is important to note that serum sodium level >160 mmol/L may also increase the risk of seizures.
Fluid status is also carefully monitored to avoid fluid overload. It is well known that volume expansion occurs after administration of HSS. For example, infusion of 7.5% HSS can increase intravascular volume by as much as 4 times the infused volume within minutes. This rapid volume expansion may pose risks such as acute pulmonary congestion and decompensated heart failure, although much of this is still under debate.
Elevated ICP is a life-threatening neurologic emergency. The administration of HSS undoubtedly has its benefits; however, kidney injury and electrolyte imbalances among neurocritically ill patients are also fairly common. Although the data on HSS and hyperchloremia among these patients are still lacking, the available data on hyperchloremia among critically ill patient populations show that this should not be disregarded.
Close monitoring of not just sodium, but chloride, blood pH, and kidney function may need to be done during prolonged HSS infusions.
Isabelle Dominique Tomacruz, MD
Nephrology Fellow
Philippine General Hospital, Manila, Philippines
@DTomacruzMD