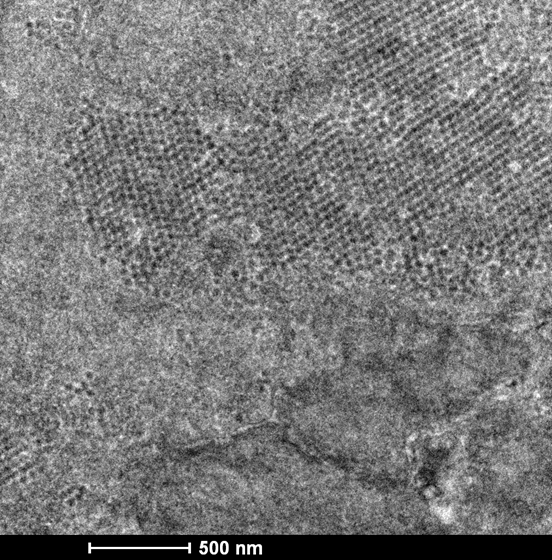
In 1971, a group of virologists in London first described a novel polyomavirus they discovered in the urine and urothelial cells of a kidney transplant recipient who had developed ureteric stenosis. Named after the patient it was first described in, this novel polyomavirus was dubbed BK virus.
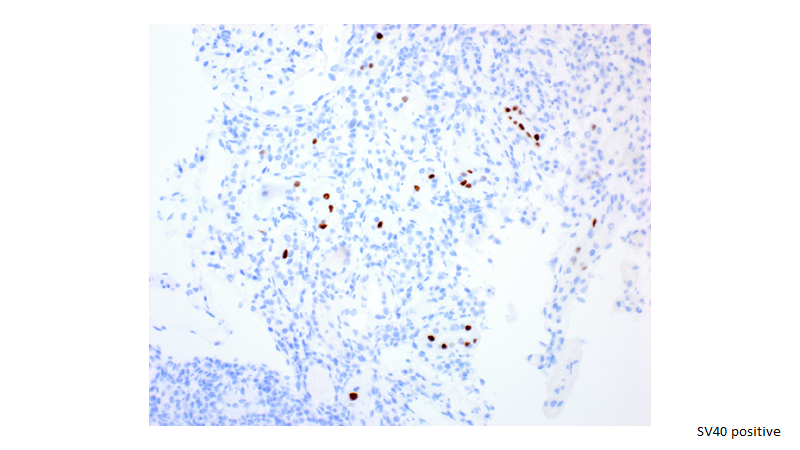
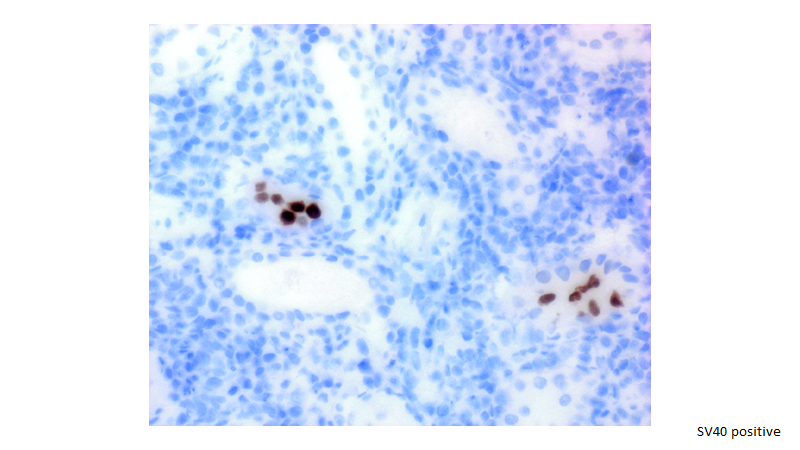
BK virus is a polyomavirus coincidentally discovered the same year as the second major polyomavirus found to infect humans, JC virus, which infects brain tissue in progressive multifocal leukoencephalopathy (and also given the initials of the patient it was first described in). For many years, these were the only two polyomaviruses known to mainly infect humans, though multiple additional human polyomaviruses have been identified since 2007 (many without known associated disease). Other polyomaviruses infect animals, notably Simian virus 40 or SV40 discovered in the kidneys of rhesus monkeys. BK virus and SV40 share 70% homology and have a common antigen, “SV40 T antigen”, allowing immunohistochemical staining for SV40 to be used to detect BK virus.
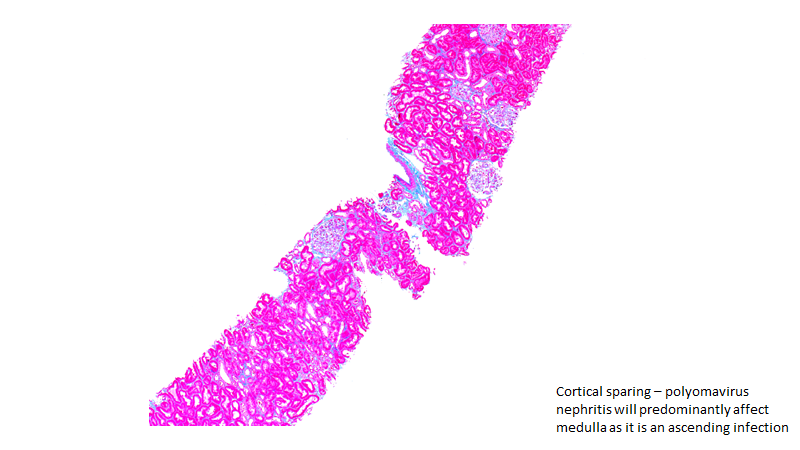
BK virus is a ubiquitous organism, with ~80% of the general population having been infected by it at some point. Primary infection is spread by respiratory secretions or urine in childhood, and manifests as mild respiratory symptoms. BK virus then becomes latent in renal tubular epithelial cells and is reactivated in the setting of immunocompromise. When reactivated, there is tubular cell lysis and viruria, with infected epithelial cells detectable in urine.
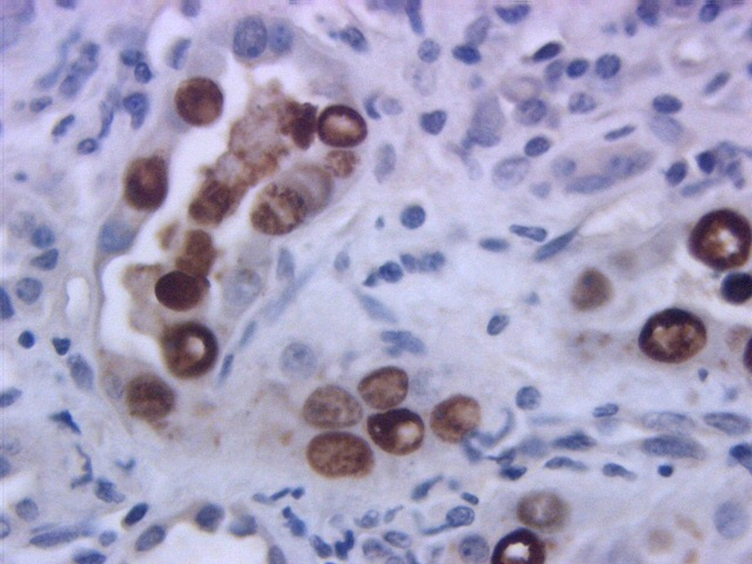
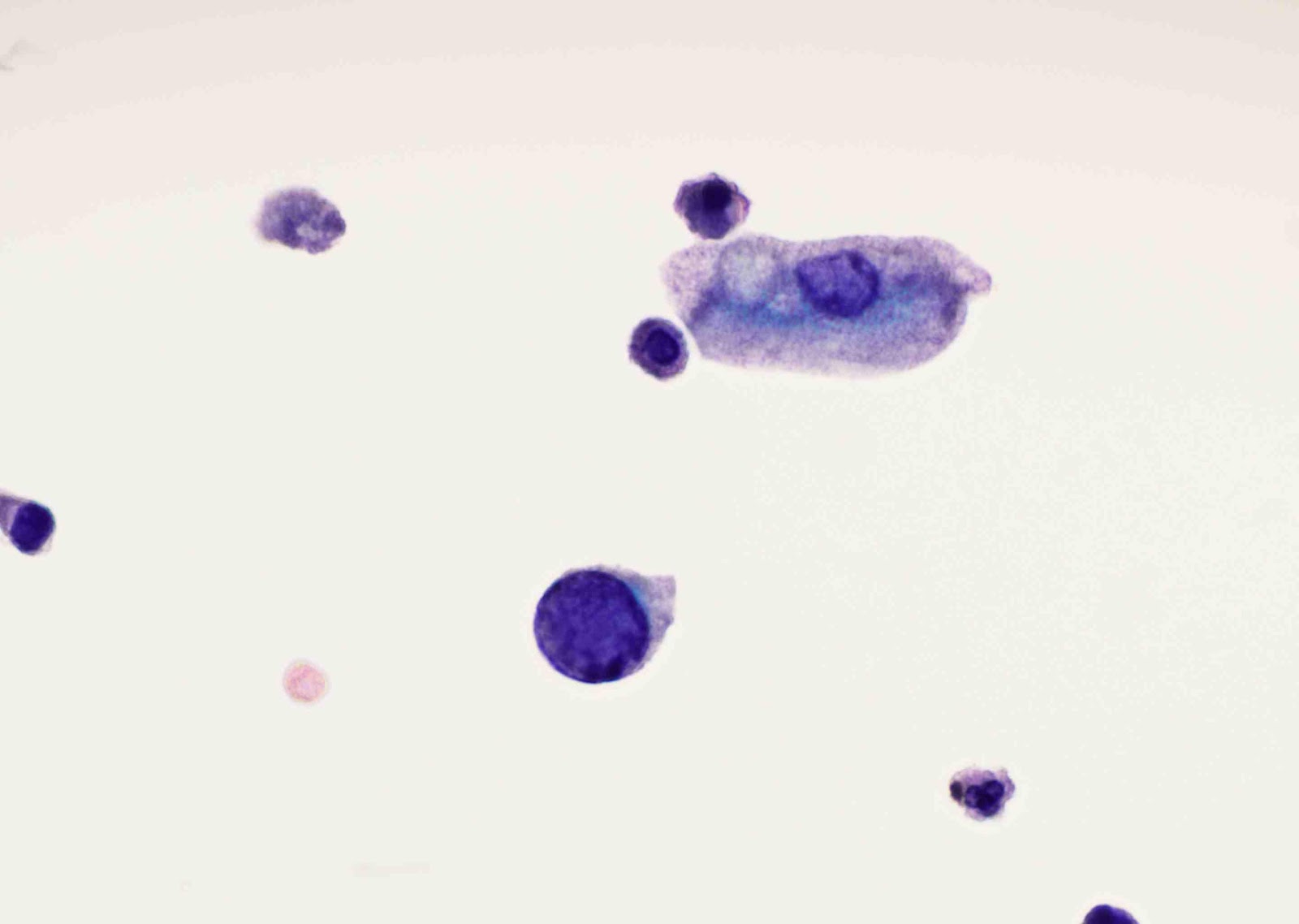
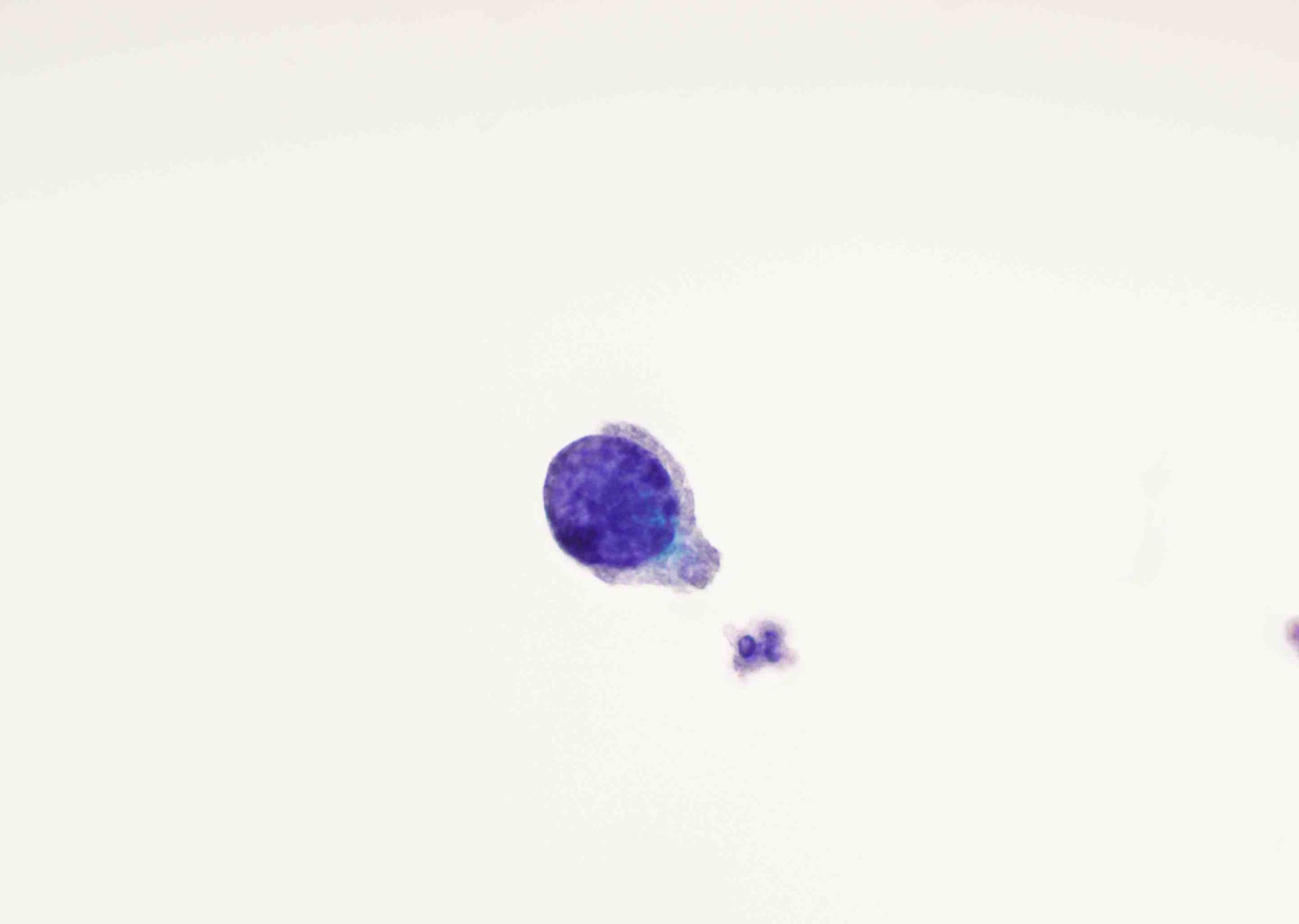
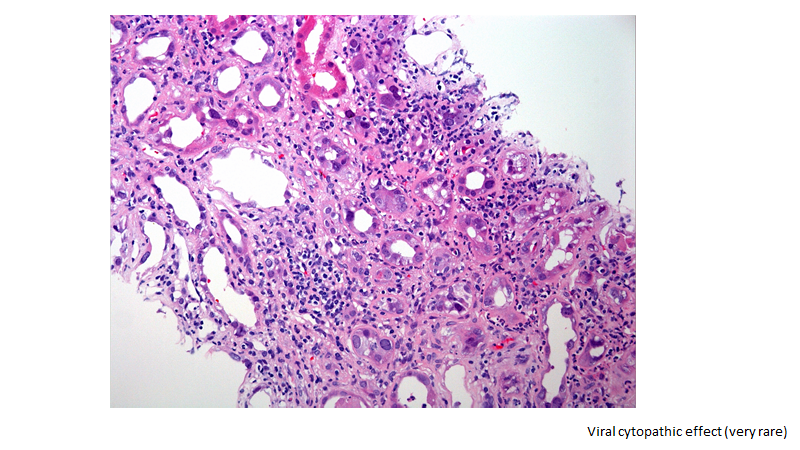
Infected epithelial cells contain intranuclear viral inclusions which may resemble malignant cells, and so have subsequently been termed ‘decoy cells’ when found in the urine. Urine cytology identifying high numbers of decoy cells is more sensitive than histology in detecting BK virus nephropathy with a negative predictive value of 99%.
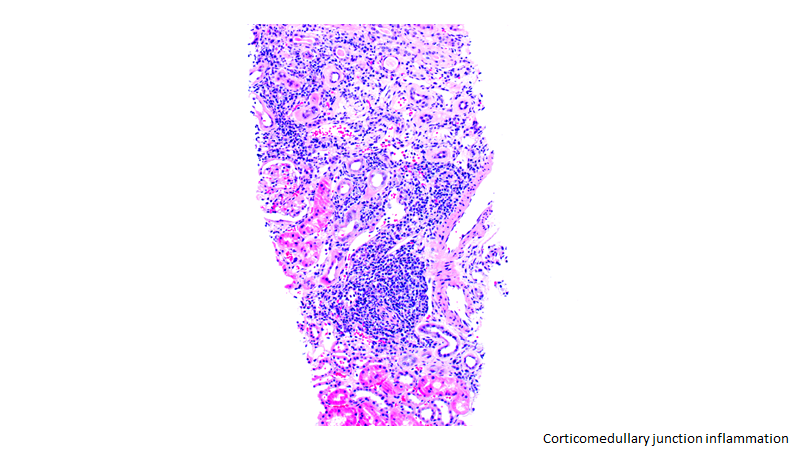
Along with reactivation in tubular epithelial cells, BK virus also multiplies in the interstitium causing tubulointerstitial inflammation which may progress to interstitial fibrosis and tubular atrophy. BK virus eventually crosses to peritubular capillaries, causing BK viremia in ~⅓ of kidney transplant recipients with viruria.
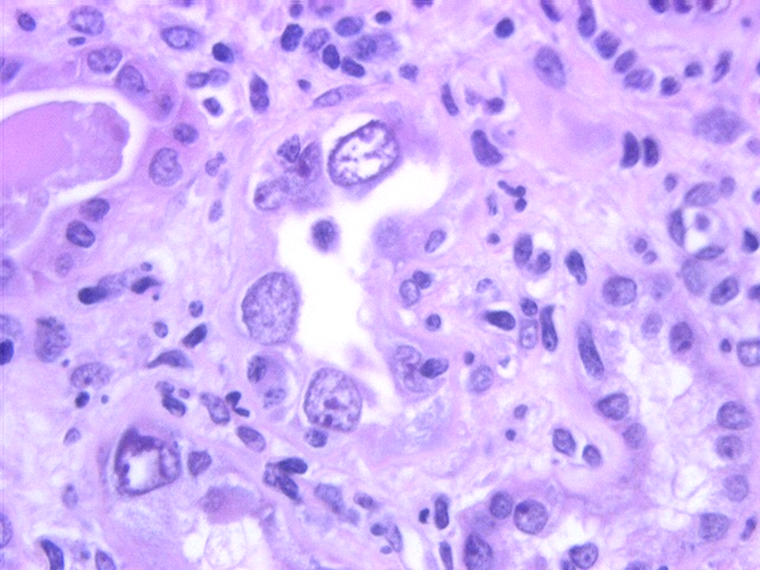
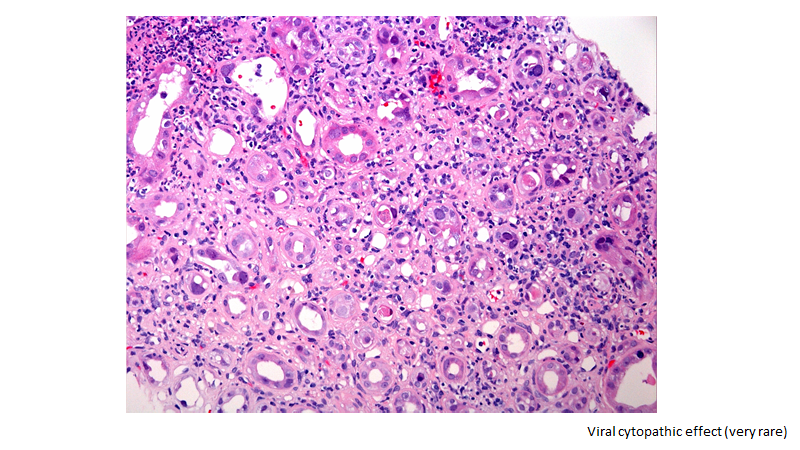
On kidney biopsy, BK virus nephropathy (BKVN) is characterized by an inflammatory lymphocytic infiltrate which can appear similar to acute cellular rejection. Intranuclear BK virus inclusion bodies staining positive for SV40 T antigen can be seen in tubular epithelial cells. However, biopsy findings can be focal so a negative biopsy cannot completely rule out early BKVN.
When BKVN is diagnosed on kidney biopsy, histologic findings can be used to prognosticate. Multiple histologic grading systems have been developed to classify the severity of BK virus nephropathy, with degree of fibrosis and tubular atrophy being most predictive of allograft outcome.
Beside BK virus nephropathy and ureteral stenosis, BK virus can also cause hemorrhagic cystitis (notably in hematopoietic cell transplant recipients).
Screening for BK virus is recommended in kidney transplant recipients. KDIGO recommends monthly plasma screening for the first 3‐6 months post‐transplant, then every 3 months until the end of the first transplant year. 2019 AST guidelines recommend monthly plasma screening for the first 9 months, then every 3 months thereafter for the first 2 years post‐transplant9.
The mainstay of treatment for BK virus nephropathy is a reduction in immunosuppression. AST guidelines recommend calcineurin inhibitor dose reduction by 25%‐50% either before or after a 50% reduction in the antiproliferative agent, and a final step of discontinuation of the antiproliferative agent if needed.10 Other adjunctive treatments may be used including cidofovir, leflunomide, quinolones and IVIG.
Tiffany Truong
Nephrology Fellow, University of Southern California