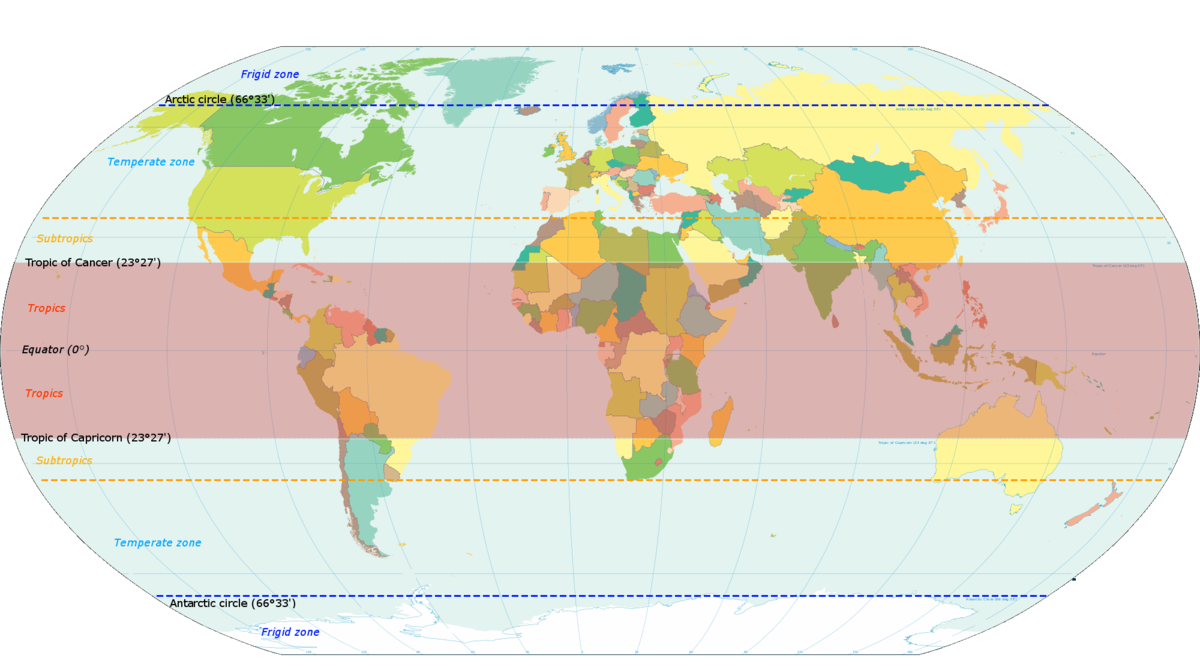
What comes to the mind when someone mentions the tropical regions of the world (Figure 1)? Evergreen forests humming with life – a veritable treasure trove of flora and fauna, a region where the sun always shines benevolently down, basking people with its warmth and glory, friendly locals who are always happy to help and perhaps a lazy day under the shade of a palm tree with a drink in your hand, just watching time go by. Doesn’t it seem like a vacation in paradise?
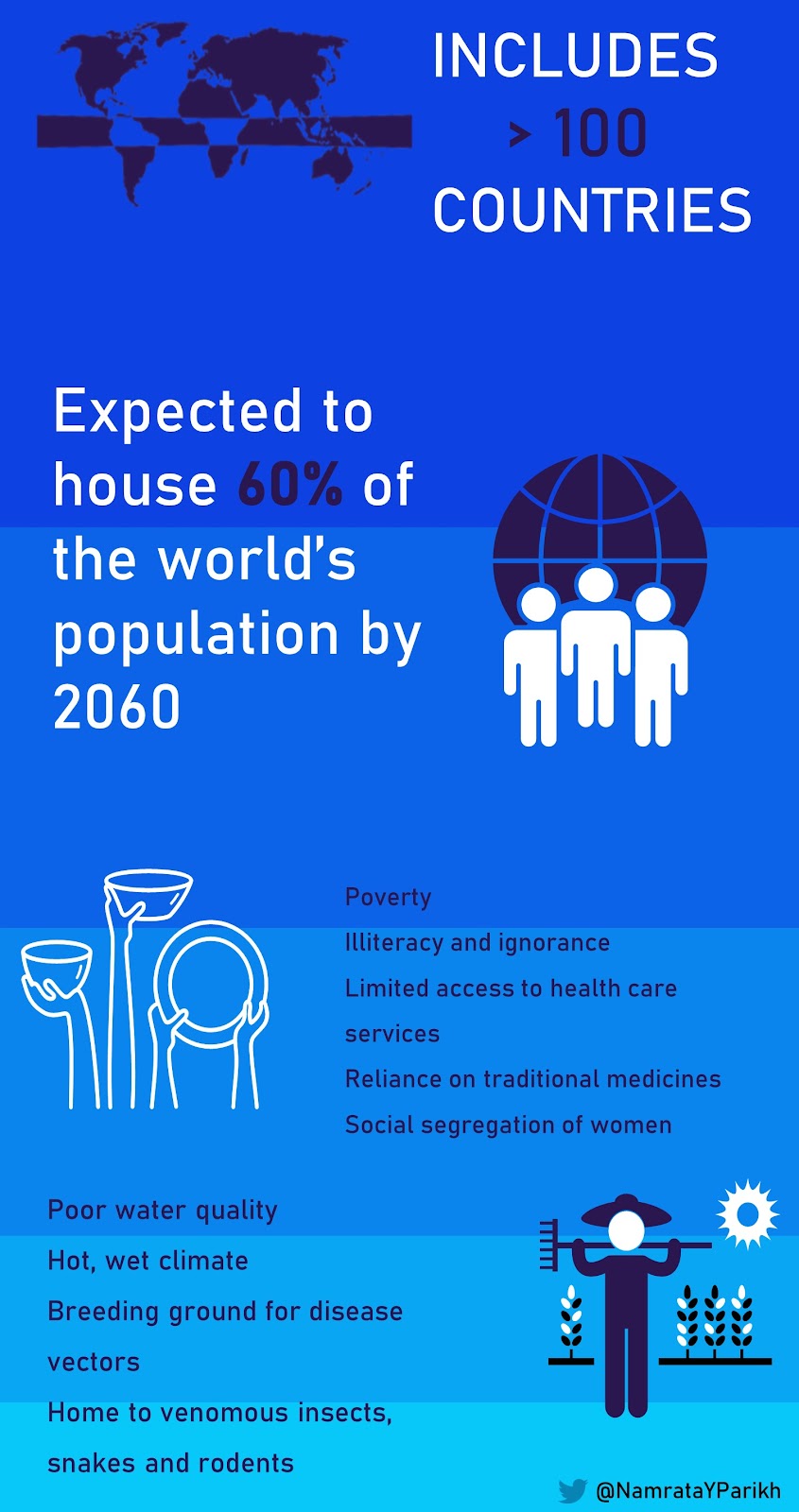
Now let me paint another picture for you – imagine extreme heat and humidity, having poor quality of water which is not fit for consumption or for agriculture; imagine unhygienic living conditions with overcrowding, having no education, no fixed source of income and almost no access to health care; imagine sharing your living space with blood-thirsty mosquitoes, hungry rodents, venomous snakes and who knows what else and at the same time being unable to procure even the most basic of antibiotics. No longer paradise, right?
Unfortunately, the latter scenario is the harsh reality for people living in the tropics – A region composed of >100 countries between the tropic of cancer and the tropic of capricorn. This region is home to roughly 40 % of the world’s population, a figure which is expected to rise to 60% by the year 2060. To make matters worse, most of the countries in this region fall within the Low Income and Low Middle Income group – with widespread poverty and an acute shortage of healthcare services (Figure 2)
As kidney care professionals, a particular area of interest for us, in the tropics, is acute kidney injury (AKI). The Kidney Disease Improving Global Outcomes (KDIGO) guidelines define AKI as any of the following:
- Increase in serum creatinine (SCr) by >= 0.3 mg/dL (26.5 micromol/L) within 48 hours OR
- Increase in SCr to >= 1.5 times baseline, which is known or presumed to have occurred within the prior 7 days OR
- Urine volume <0.5 mL/kg/hr for 6 hours
AKI in the tropics has certain distinct characteristics, which have earned it the title of ‘tropical AKI’ (tropic associated AKI or TA-AKI, anyone?).
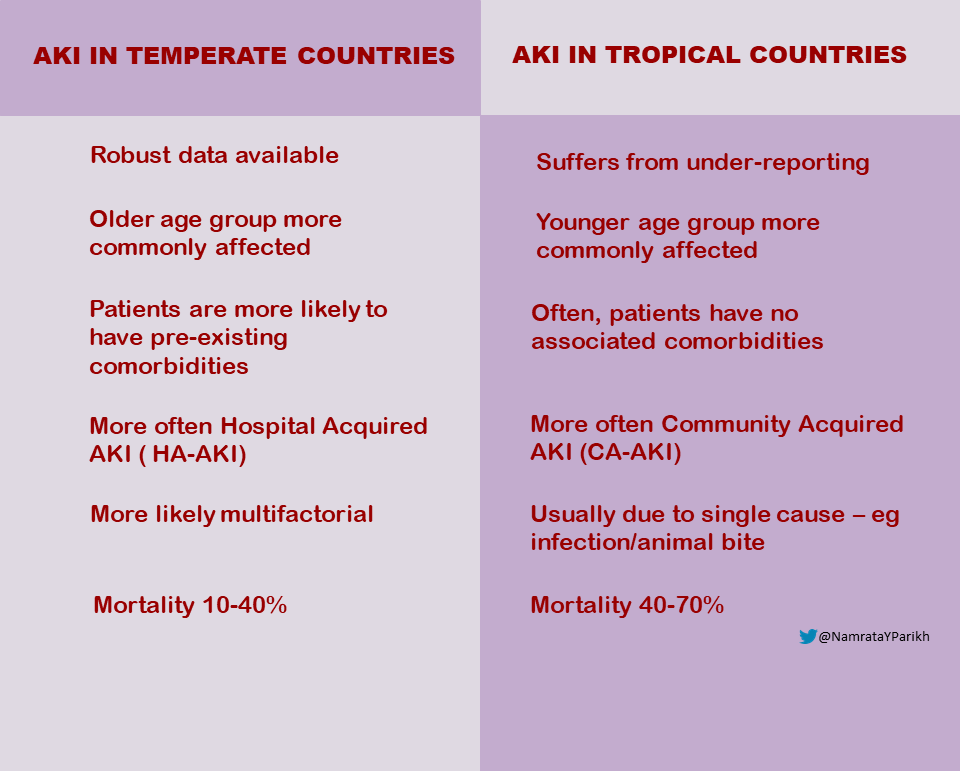
Another factor which increases the vulnerability of this region is the lack of clinical data – which at present is available only from tertiary care centers in urban areas. This means that the most severely affected population in remote regions remains grossly under-represented. As per available data, the incidence of AKI in the tropics ranges from 0.31 to 7.9 cases per thousand hospital admissions. There are also significant differences in the profile of AKI cases in tropical countries, compared to temperate countries (Figure 3).
A point to stress here is the particularly poor plight of the female population. They are poor, under-nourished, uneducated, more likely to be affected and less likely to seek or receive treatment.
It has also been observed that tropical AKI is amenable to quite simple and basic treatment. Lack of awareness among the locals and scarcity of resources is the main wrench in the system.
Etiology and pathophysiology:
Jha and Parameswaran have described tropical AKI in great detail in several publications. Adapted from their work, the etiology of tropical AKI can be grossly summarized as under (figure 4):
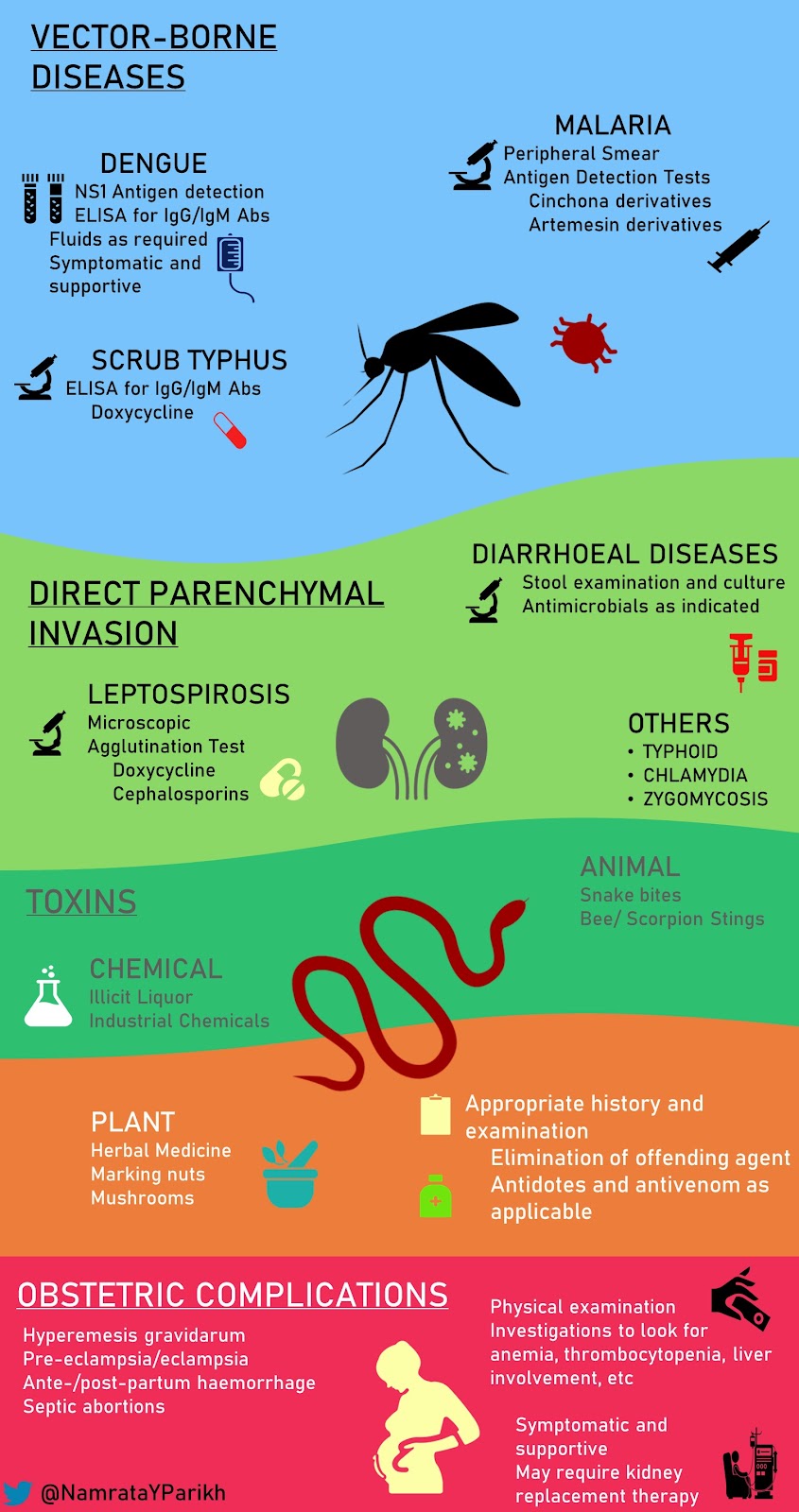
As the aetiology of tropical AKI is so diverse, it follows that the pathophysiology is also quite variable, depending upon the causative agent. Moreover, each causative agent may have multiple pathophysiological pathways, through which it produces AKI:
Direct Parenchymal Invasion
- Acute Interstitial Nephritis
- Leptospirosis (Leptospira interrogans)
- Scrub typhus (Orientia tsutsugamushi)
- Dengue (Dengue virus – various serotypes)
- Mucormycosis (Fungal – mucormycetes)
- Microabscess
- Melioidosis (Burkholderia pseudomallei)
- Solitary Abscess
- Typhoid (Salmonella typhi)
- Hemodynamic Disturbances
- Sepsis
- Disseminated intravascular coagulation
- Rhabdomyolysis
- Immunological Disturbances
- Post-infectious glomerulonephritis (Eg. Typhoid, malaria)
- Crescentic glomerulonephritis
- Hemolytic uremic syndrome (Eg. bacterial sepsis, Snake bite – particularly vipers)
- Acute Cortical Necrosis
- Obstetric complications
- Snake bite (notably Russell viper)
- Severe sepsis
- Acute Tubular Injury
- various infections may precipitate tubular damage by virtue of various inflammatory mediators, volume depletion and other mechanisms like rhabdomyolysis, disseminated intravascular coagulation, etc
Various infections may precipitate tubular damage by virtue of various inflammatory mediators, volume depletion and other mechanisms like rhabdomyolysis, disseminated intravascular coagulation, etc
Management:
The evaluation and treatment of tropical AKI depends on the suspected causative agent. AKI ‘syndromes’ described by Jha and Parameswaran may be useful in this regard. On the basis of history and clinical examination, a provisional diagnosis can be made and after confirmation with appropriate investigations, treatment can be initiated (figure 4).
Thus, AKI in the tropics has multiple mechanisms and shows diverse clinical presentations, but can be diagnosed by simple investigations and treated promptly once diagnosis is made. If picked up early, significant morbidity and mortality can be prevented.
A point worth mentioning here is that while the coronavirus infectious disease – 2019 (COVID-19) has reached pandemic proportions, countries in the tropics have some of the highest number of cases (for example, India currently occupies the second rank in the world in terms of number of active cases). This is in addition to the burden of various infections and diseases, which are endemic to these regions. As a result, the existing health care system has been put into dire straits. To describe the situation in India, the country has just finished its monsoon season with unprecedented rainfall and flooding in several regions. Dengue, malaria and leptospirosis have already started increasing, while health care professionals continue to be engaged in the battle against the COVID-19. The situation in other tropical countries is expected to be the same. One can only hope that the pandemic will relent and the availability of a vaccine will result in a fall in the number of cases.
Namrata Parikh, MD
Attending Nephrologist
Adipur, Gujarat, India
@NamrataYParikh

Brilliantly Simplified
Wonderful writing.
@md_abdulqader83
Excellent!!