Systemic glucocorticoids: an overview of side effects– Since the synthesis of cortisone in the 1950s, glucocorticoids have become a staple in the treatment of many inflammatory and autoimmune diseases and a key component of immunosuppressive combinations for transplant recipients. Over time, we have also become familiar with the slew of side effects these medications have. But before we dive into these, let’s first review how glucocorticoids work.
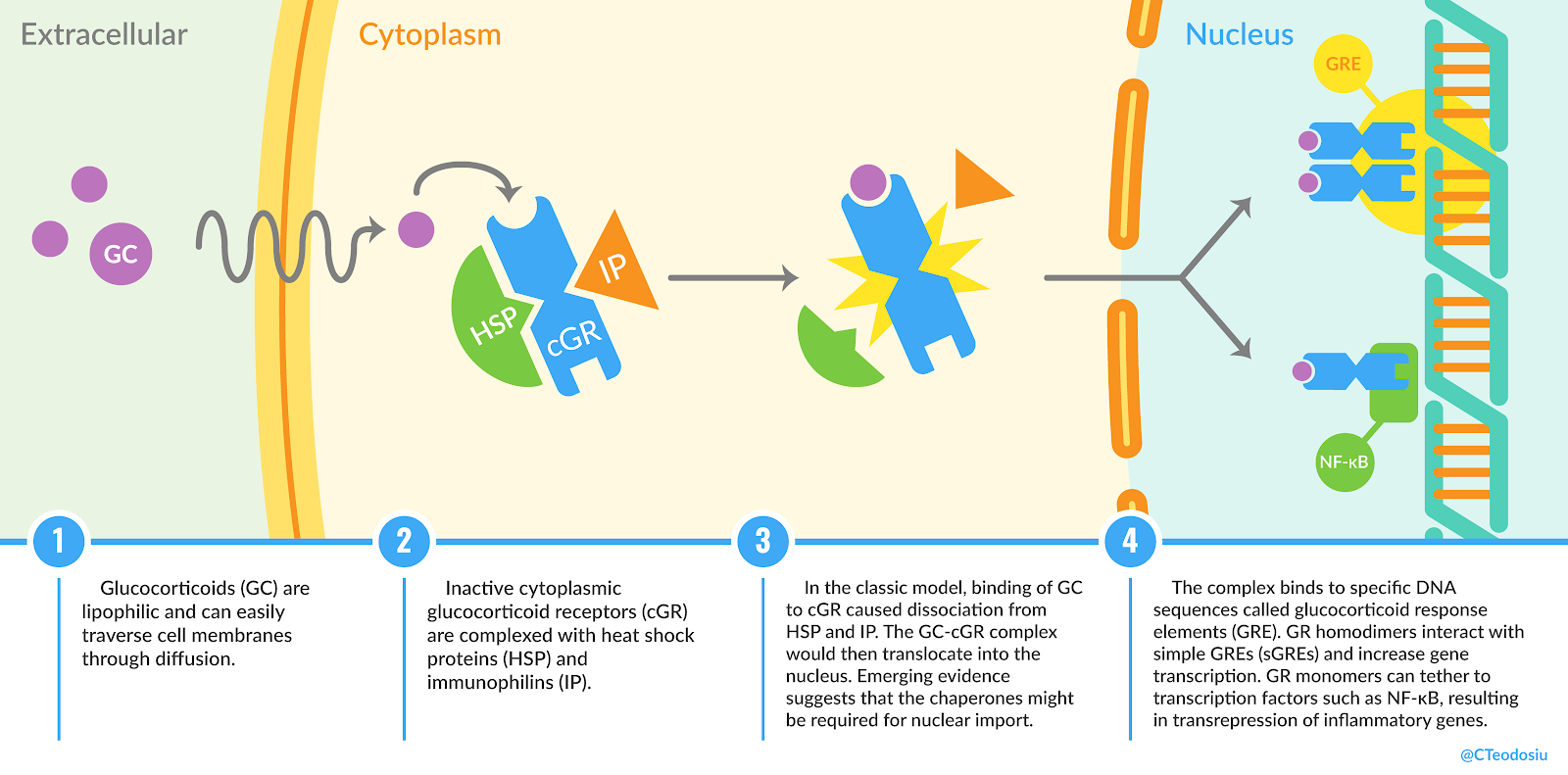
What are the mechanisms involved in adverse effects? The molecular targets of endogenous cortisol (as well as its synthetic variants) are the glucocorticoid receptors (GR), located either in the cytoplasm (cGR) or on the cellular membranes (mGR). Almost all nucleated cells possess GRs, so one can expect their results (whether desirable or not) to be quite numerous and diverse. The effects of glucocorticoids can be classified into genomic (when influencing gene transcription) and non-genomic (transcription-independent). The former occur after a delay of hours or days, while the latter arise within seconds or minutes.
When glucocorticoids bind to cGR, the resulting complex translocates into the nucleus (Figure 1) where it produces genomic effects. Some nuclear signaling pathways involve homodimerization of the GR complex and binding to glucocorticoid response elements (GRE) in the DNA, which leads to increased gene transcription (transactivation). In other pathways, monodimeric GR binds to negative GREs or tethers transcription factors, such as nuclear factor-kB (NF-kB) and activator protein 1, inhibiting gene transcription (transrepression). Tethering is believed to be responsible for the clinically desirable outcomes, such as reduced synthesis of proinflammatory proteins. Hypothetically, compounds that specifically engage into transrepression would retain their anti-inflammatory properties while becoming free of the side effects generated by transactivation. However, some undesirable effects (such as osteoporosis and hypothalamic-pituitary-adrenal (HPA) insufficiency) appear to be mediated by transrepression, and some immunosuppressive effects may be due to transactivation. The concept of selective glucocorticoid receptor agonists and modulators is currently under study.
On the other hand, non-genomic effects are usually the result of interactions with cGR, mGR or with the cellular membranes themselves. These are generally poorly understood; some involve increased nitric oxide generation and signaling, while others act on inflammatory pathways such as those promoted by mitogen-activated protein-kinases (MAPK).
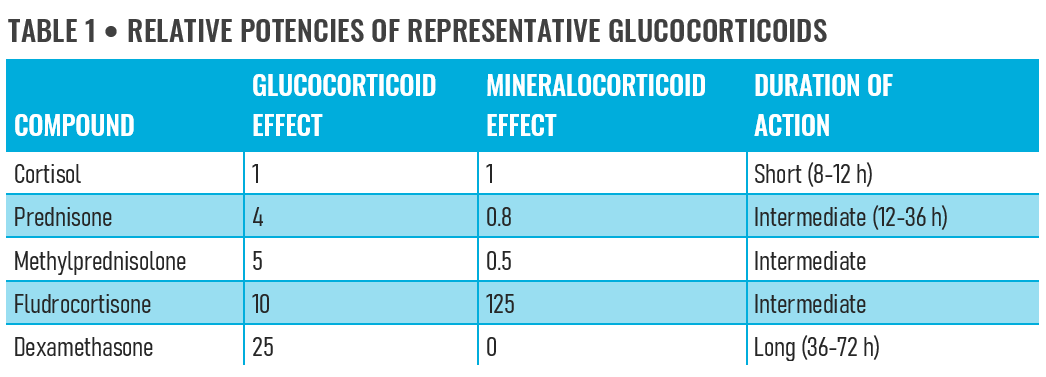
Unlike endogenous cortisol, most synthetic glucocorticoids are designed to not exhibit significant mineralocorticoid effects (such as sodium and water retention). Instead, they are engineered to be more potent immunomodulators through their extended half-lives and increased affinities for GRs. Additionally, synthetic variants cannot attach to corticosteroid-binding globulin and thus circulating levels are not influenced by the degree of protein binding. There are a number of glucocorticoid analogues, each with different potencies relative to cortisol (see Table 1).
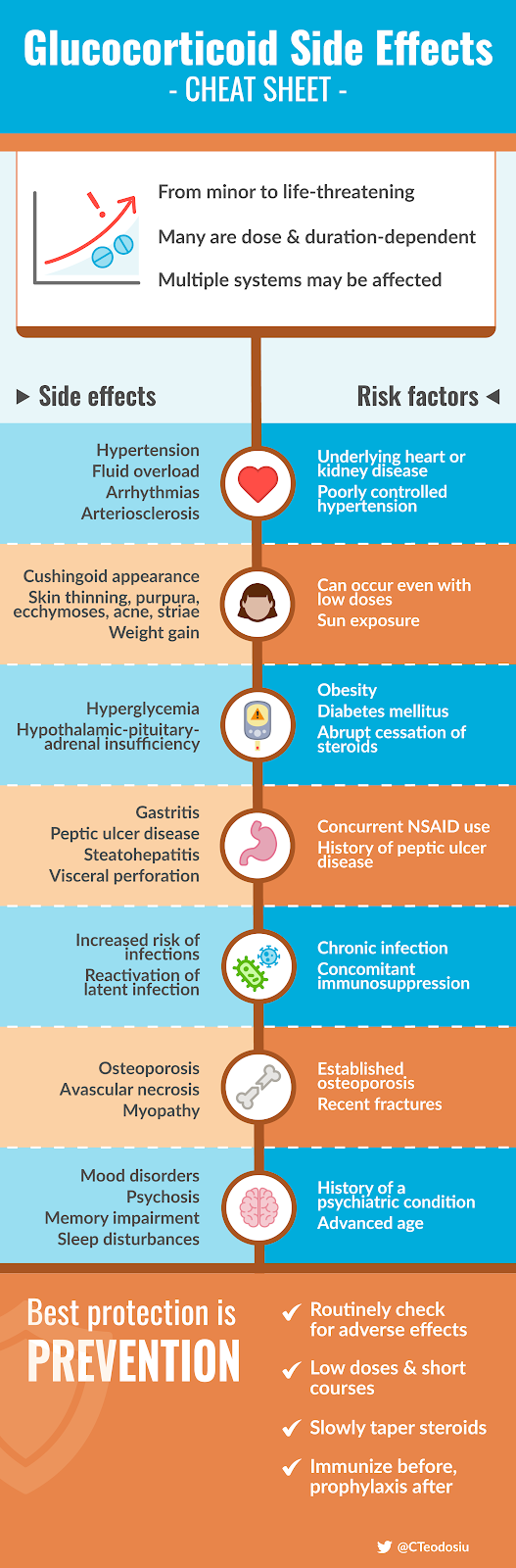
What are the side effects? The undesirable effects of glucocorticoid use can range from generally benign issues (but potentially displeasing for patients, such as acne and hirsutism) to life-threatening conditions (eg, sepsis). Most of these tend to occur in a dose- and duration-dependent manner; higher doses and longer treatment periods are associated with increased incidence of side effects. Additionally, some of them may not be clinically manifest until further complications occur (such as bone fractures due to glucocorticoid-induced osteoporosis).
- Cardiovascular:
- hypertension is a relatively common side effect even when the administered glucocorticoids lack appreciable mineralocorticoid activity
- atherosclerotic disease
- arrhythmias (atrial fibrillation and flutter)
- peripheral edema
- Gastrointestinal:
- gastritis, peptic ulcer and gastrointestinal bleeding are more frequent when glucocorticoids are used together with NSAIDs
- visceral perforation
- hepatic steatosis
- Immune:
- increased risk of infections (especially when combined with other immunosuppressive therapies or when there is preexisting lymphopenia or diabetes)
- progression of latent infection (such as tuberculosis, hepatitis B and C)
- leukocytosis (check out the excellent tweetorial by @tony_breu for the mechanisms behind this side effect!)
- Endocrine and metabolic:
- hyperglycemia and worsened glycemic control in diabetic patients
- glucocorticoid-induced diabetes is more likely to occur in patients with predisposing conditions such as old age, family history of diabetes, hypertension and obesity
- HPA insufficiency when glucocorticoids are withdrawn abruptly
- weight gain and Cushingoid features
- Neuropsychiatric:
- mood disorders (ranging from euphoria to depression) are more likely to occur in patients with a history of alcohol abuse or psychiatric condition
- psychosis
- Musculoskeletal:
- osteoporosis, which tends to affect trabecular bones (such as the vertebrae or the femoral head) and increases the risk of low-energy fractures
- osteonecrosis
- myopathy
- growth cessation in children
- Dermatologic:
- skin thinning and atrophy
- striae
- ecchymoses
- hirsutism
- acne
- Ophthalmologic:
- cataract
- glaucoma
How can we reduce side effects? Before starting treatment, it is recommended to assess risk factors such as the ones listed in Figure 2. Depending on these risk factors, patients should be monitored during treatment for changes in blood pressure, glycemia, serum lipids, peripheral edema, and ocular pressure. In general, one should aim for the lowest possible dose and shortest period of time required to achieve treatment goals. Slowly taper glucocorticoids especially when HPA suppression is likely (patients with Cushingoid appearance, use of prednisone doses greater than 10 mg/day or bedtime administration of more than 5 mg of prednisone longer than 3 weeks). There are some exceptions – abrupt discontinuation is necessary in patients with acute psychosis (when unresponsive to antipsychotic medication) or herpesvirus-induced corneal ulceration (which can quickly progress to blindness).
Depending on the patient and treatment profile, consider specific prevention strategies such as:
- When the treatment duration exceeds 3 months, ensure an intake of vitamin D of 600-800 IU/day and a total calcium intake of 1000-1200 mg/day (either through diet or supplements).
- In patients at risk of gastrointestinal bleeding, consider using histamine-2 receptor antagonists or proton pump inhibitors.
- In children over 6 months old with CKD stages 3-5D and persistent growth failure (defined as height under the 3rd percentile for age and sex and a height velocity below the 25th percentile), consider replacement therapy with recombinant growth hormone to reduce the impact of glucocorticoid-induced growth suppression.
- Address vaccination deficiencies – in particular live vaccines should be administered 2-4 weeks before starting therapy.
- Use pneumocystis pneumonia prophylaxis in susceptible patient populations (eg. kidney transplant recipients or patients receiving high dose glucocorticoids and additional immunosuppressive medication). More information on whether prophylaxis should be started for patients on glucocorticoids alone will likely be revealed when the results of the TESTING trial are out.
Corina Teodosiu, MD
Nephrology Fellow (NSMC intern 2020)
Bucharest, Romania
@CTeodosiu