Clayton Brady
MD/PhD Candidate (G2)
University at Buffalo Jacobs School of Medicine and Biomedical Sciences
Acid-base balance is often overlooked in healthy individuals, but becomes glaringly important in any patient with reduced kidney function. Our kidneys do a tremendous job of maintaining blood pH within its narrow constraints; combatting a daily acid-load that is primarily from dietary protein intake, through production of an equivalent amount of “new” bicarbonate. Patients with CKD however, cannot keep up with this daily acid-load. This leads to the development of acidosis that has detrimental effects on just about every organ system you can think of. This includes bone and muscle wasting, impairments in cardiac contractility and increased risk of cardiovascular disease, as well as inappropriate changes in hormone release and signaling. Intuitively, it makes sense to supplement these patients with bicarbonate, and this is exactly what clinical researchers have been testing over the past few years. Surprisingly, it was found that bicarbonate therapy didn’t just help prevent the detrimental effects of acidosis on other organ systems; it may actually slow the progression of kidney disease itself. Thus, acidosis is not only caused by CKD, but is possibly a contributor to disease progression as well. Furthermore, other data indicates that higher bicarbonate levels within the normal range (20-30 mEq/L) are associated with better kidney outcomes (slower GFR decline and longer time to dialysis). This further supports the idea that bicarbonate supplementation is beneficial in CKD patients, even in patients without acidosis. This link between kidney health and bicarbonate has opened the door for basic science to provide insight into these unexpected but exciting clinical observations.
In order to understand how bicarbonate helps “protect” the kidney, we first have to understand how the kidney deals with an acidosis. The primary response of the kidney to acidosis is an upregulation of the metabolic process of ammoniagenesis, so named because it produces ammonia from the amino acid glutamine (Figure 1A). While the name clearly puts emphasis on ammonia production, ammoniagenesis produces “new” bicarbonate as well, which is actually the more important feature of ammoniagenesis in terms of acid base balance. The ammonia gets excreted in the urine, while the bicarbonate is transported into the blood where it replenishes the plasma buffer system. Of note, ammonia exists in two molecular forms: ammonia (NH3) and ammonium (NH4+), however for simplicity, here “ammonia” refers to the combination of both molecular forms NH3 and NH4+.
This ammoniagenic response to acidosis appears to be at the center of the mechanism regarding how acidosis damages the kidney. It is postulated that increased ammoniagenesis leads to ammonia deposition in the interstitium, which triggers complement activation and ultimately leads to interstitial fibrosis. This could explain why bicarbonate therapy might be beneficial even to individuals in the early stages of CKD who do not have overt acidosis. Due to their mild kidney disease, these patients may have lost ammoniagenic capabilities in some nephrons. However, they are still able to adequately maintain overall pH due to upregulation of ammoniagenesis in their remaining functional tubules. The problem is that this upregulation may promote ammonia retention leading to intrarenal inflammation that hastens CKD progression. Thus, in this situation bicarbonate supplementation may act to inhibit this ammoniagenic response and therefore help slow the progression of kidney disease. While this is an intriguing hypothesis, a major gap in the field is that how the kidney actually senses changes in blood bicarbonate concentrations and responds with changes in ammonia production remains unknown. To this end, recent basic science research has demonstrated a link between kidney bicarbonate transport and ammonia handling that may help partly explain this effect of bicarbonate therapy on ammonia production.
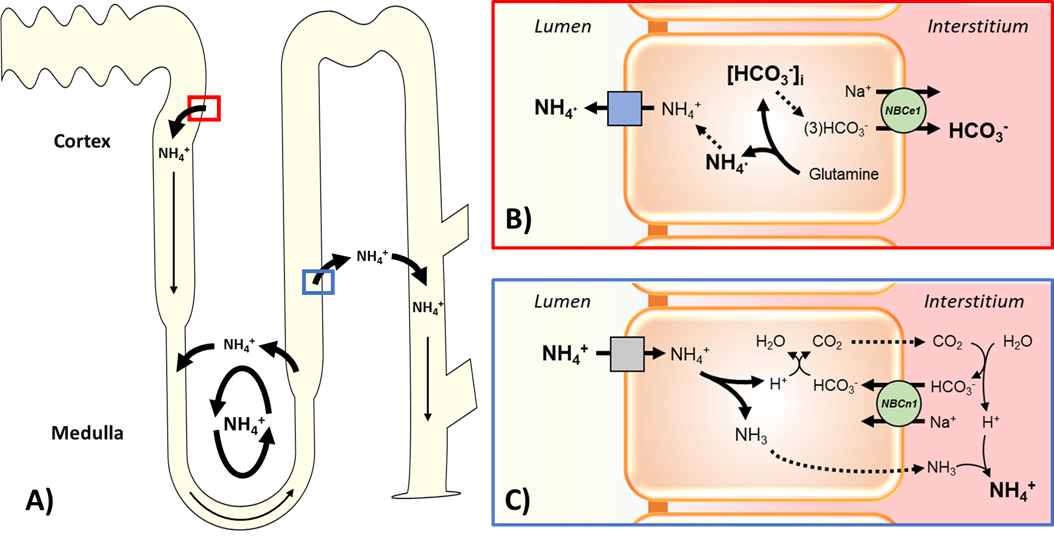
The electrogenic sodium-bicarbonate cotransporter, NBCe1, is the transporter in the proximal tubule that is responsible for exporting bicarbonate produced by ammoniagenesis into the blood (Figure 1B). Studies by Handlogten et al. and Lee et al. demonstrated that NBCe1 is essential for the coordinated upregulation of all the enzymes necessary for the ammoniagenic response. This result implicates bicarbonate transport as the upstream “effector” that regulates ammoniagenesis. Thus, even in normal pH balance, bicarbonate administration may diminish the driving force for this transport activity, and consequently decrease ammonia production and prevent damaging inflammation. More recently, Olsen et al. investigated the role of the electroneutral sodium-bicarbonate cotransporter, NBCn1, in the transport of ammonia from the lumen of the thick ascending loop of Henle to the medullary interstitium. They demonstrated that NBCn1-mediated basolateral bicarbonate influx neutralizes the intracellular acidification that would otherwise inhibit ammonia excretion (Figure 1C). In this situation, bicarbonate administration would actually promote ammonia export into the interstitium. At first glance this would presumably lead to more ammonia deposition and inflammation. This may very well be true in patients with CKD, who have a decrease in functional kidney mass, but have compensatory increases in single nephron ammonia production. However, in individuals without CKD and enough kidney mass to support the increased flux in ammonia through the kidney interstitium and into the collecting duct, this effect of bicarbonate on NBCn1 may increase overall ammonia excretion. This would help prevent a build up of ammonia in the kidney and maintain acid-base balance. Extrarenal mechanisms may also underlie the beneficial effect of bicarbonate in CKD; an idea supported by evidence that bicarbonate activates the cholinergic anti-inflammatory pathway that dampens harmful inflammation in the kidney.
Summary
- The buildup of ammonia in the kidney interstitium may lead to kidney inflammation and faster CKD progression.
- Ammoniagenesis in the proximal tubule requires the bicarbonate transport activity of NBCe1.
- Bicarbonate transport via NBCn1 is essential for the movement of ammonia from the lumen of the thick ascending limb into the interstitium, which is necessary for the ultimate secretion of ammonia into the collecting duct and excretion from the body.
- Bicarbonate supplementation may lessen ammonia production and improve the efficiency of ammonia transport, ultimately helping protect the kidney from the harmful effects of metabolic acidosis.
Overall, understanding the details of ammonia handling by the kidney and determining how this transport is affected in the setting of kidney disease is essential for the development of future therapies to treat the detrimental effects of CKD. It is exciting to envision a treatment paradigm that could bolster ammoniagenesis early in disease, in order to promote acid-excretion and maintain proper pH balance. Later in disease, treatment could aim to inhibit the ammoniagenic response as a means to prevent the harmful effects of ammonia deposition in an already injured kidney, while concomitant increases in alkali therapy would still help maintain overall blood pH. Clearly, a multifaceted approach is warranted, with basic science research capable of laying the groundwork for an entirely novel therapeutic strategy for the treatment of CKD.
Reviewed by: Elinor Mannon, Kelly Hyndman, PhD, and Matthew Sparks, MD, FASN, FAHA
If you enjoyed reading this post and want to learn more about the use of alkali in CKD and ammonia handling by the kidney, considering checking out these posts:
From the Nate Hellman Unpublished Archive: Renal Ammonia Handling