Carlo Trinidad, MD
Nephrologist
Dagupan Doctors Villaflor Memorial Hospital, Philippines
@hellokidneyMD
Diuretic resistance is defined as the failure to achieve the desired diuresis (with concomitant reduction in edema and/or congestion) despite maximal doses of diuretic (Hoorn et al. American Journal of Kidney Diseases. 2017). It represents a significant challenge in the management of acute decompensated heart failure (ADHF). Several mechanisms have been suggested in the development of diuretic resistance.
Short-term tolerance to loop diuretics develops due to renin-angiotensin aldosterone system and sympathetic nervous system activation from acute sodium and water loss. This results in renal vasoconstriction and increased sodium absorption along the proximal convoluted tubule. (Burnier and Brunner. European Heart Journal.1992). Aldosterone likewise increases, causing sodium reabsorption along the distal nephron as well. Short-term compensatory mechanisms such as post-diuretic sodium retention can be overcome by increasing the dose and/or frequency of loop diuretics (Hoorn et al. American Journal of Kidney Diseases. 2017). However, in patients already on chronic loop diuretic treatment, there is another mechanism literally putting the brakes on any attempts to diurese effectively.
Enter the braking phenomenon, a diuretic resistance mechanism brought about by the combination of chronic adaptive hemodynamic and structural changes, specifically in the distal nephron (Casu and Merella. European Cardiology Review. 2015). These changes bring about a blunted natriuretic response to loop diuretic during repeated administration (Unwin et al. Clin Sci Lond .2000). What gives rise to this diminishing diuretic efficacy?
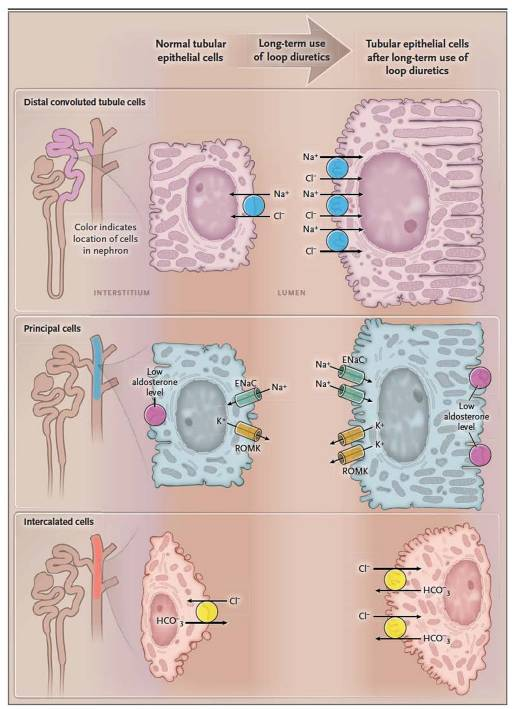
Kaissling et al. first demonstrated the braking phenomenon in rats, wherein prolonged infusions of loop diuretics caused significant hypertrophy of their distal convoluted tubules, connecting tubules and intercalated cells of their collecting ducts. This distal nephron remodelling is further amplified by increased angiotensin II and aldosterone concentrations brought about by chronic diuretic administration (Weisser and Ripka. Journal of Cardiovascular Pharmacology. 1992 ). Recent studies have shown the contribution of loop diuretic-induced chloride depletion in diuretic braking (Berend et al. Eur J Intern Med. 2012). Hypochloremia causes increased WNK1 and WNK4 activity, resulting in the stimulation of both NKCC2 (Na-K-Cl cotransporter) and NCC (Na-Cl cotransporter) (Cuthbert et al. Cardiol Ther. 2020). All of these result in an increased reabsorption of sodium in the distal nephron, diminishing the natriuretic response.
The key to breaking the braking phenomenon is plugging all the “holes” along the nephron where sodium might escape and be reabsorbed. Sequential nephron blockade by combining diuretics acting on different segments of the nephron counters the escape of sodium to the distal segments (Knauf and Mutschler. J Cardiovasc Pharmacol. 1997). The logical choice to be the partner for loop diuretics are a thiazide or thiazide-like diuretic. Combination therapy with these agents have been shown to be highly effective in inducing diuresis among patients with loop diuretic resistance (De Bruyne. Postgrad Med J. 2003). The addition of a distally acting diuretic produces significant improvement in diuresis among those already resistant to high doses of loop diuretics. This diuretic synergism extends even in those with advanced kidney failure (Fliser et al. Kidney Int. 1994).
Metolazone has often been the popular choice to combine with furosemide, owing to its oral route of administration, long half-life and its high efficacy even in patients with advanced kidney disease. However, there is no clear evidence of superiority of thiazide/thiazide-like diuretic over another and other members of this drug class may be equally effective (Ellison. CJASN. 2019). The 3T Trial showed that metolazone, chlorothiazide and tolvaptan are equally effective in inducing 48 hour weight loss when combined with high dose furosemide infusion (Cox et al. J Am Coll Cardiol HF. 2020).
How do we go about starting our sequential nephron blockade? A good starting point would be the algorithm shown below, which was adapted from the CARRESS-HF trial. This escalating dose approach has been shown to be similar in efficacy with ultrafiltration (Bart et al. N Engl J Med. 2012).
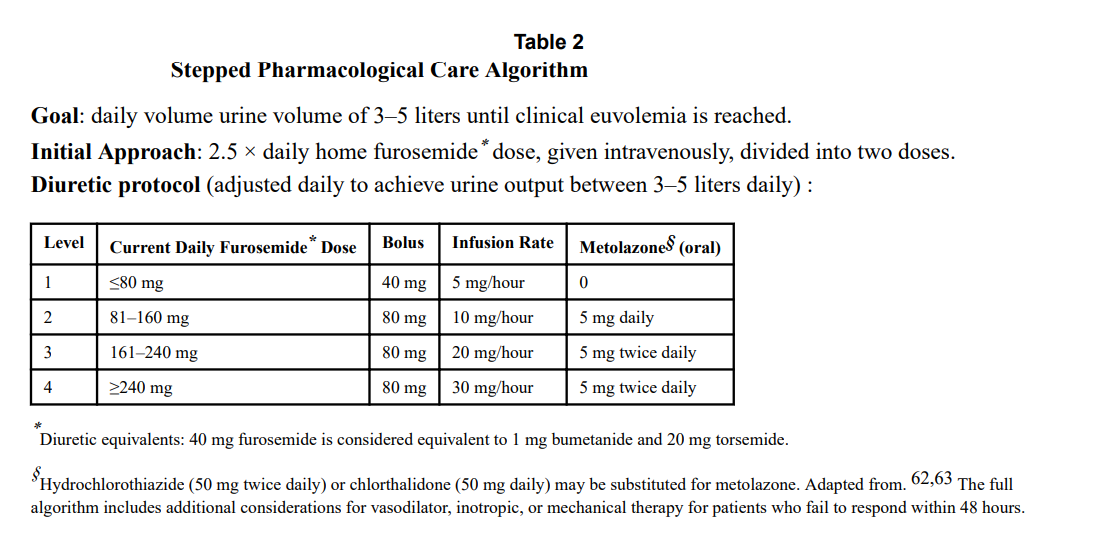
Because of metolazone’s much longer half life (14 hours), maximizing nephron blockade theoretically rests on giving it some time before loading furosemide. This ensures that the distal nephron is blocked by the time furosemide causes increased sodium delivery to the DCT. There is no evidence with regards to the optimal timing of metolazone administration prior to furosemide and in the grand scheme of things may not matter as much owing to its long half-life.
Other drug classes remain situational picks in combined diuretic therapy. Spironolactone is less useful in ADHF but is a great choice for patients with chronic HF or ascites from cirrhosis. Acetazolamide can be used to correct metabolic alkalosis brought about by loop diuretics and may have increased utility in patients with HF with concomitant sleep apnea. Tolvaptan is approved for the treatment of hypervolemic and euvolemic hyponatremia in HF and SIAD. SGLT2 inhibitors are a new drug class that may well be diuretic enablers that have synergistic action with loop diuretics. A recent study (Griffin et al. Circulation. 2020) showed that empagliflozin causes significant natriuresis when combined with loop diuretics. This natriuresis however was not associated with neurohormonal activation commonly seen in loop diuretic monotherapy.
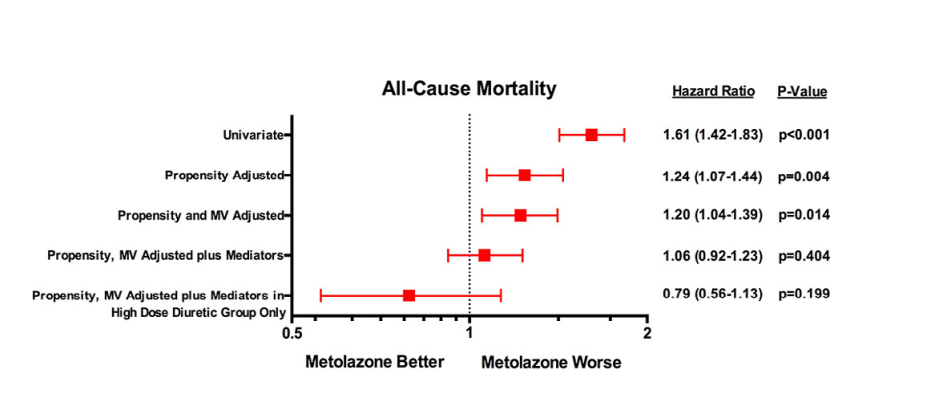
Combination diuretic therapy is not without its drawbacks. Hyponatremia, hypokalemia and volume depletion are some of its more common adverse effects. In a study among ADHF patients who received IV loop diuretics, concomitant metolazone use was associated with increased mortality, mediated by diuretic-induced hyponatremia, hypokalemia and worsening kidney failure (Brisco-Bacik et al. J Am Heart Assoc. 2018). These adverse events may further be aggravated by low kidney function, hence caution should be observed and the necessary dosing frequency adjustments be made when using metolazone in patients with CKD.
Diuretics remain as one of our most powerful tools in the management of fluid overload in different clinical settings. The development of diuretic braking leading to resistance represents a major hindrance in the management of the congested and oliguric patient. Using the entire nephron with combination diuretic therapy can overcome diuretic braking without having to subject the patient to a more invasive (but not necessarily superior) therapy like ultrafiltration. Individualizing combination diuretic therapy will help mitigate the adverse effects associated with multiple diuretic use.
Reviewed by Matthew A. Sparks, Amy Yau, Caitlyn Vlasschaert

Hitting the nail on the head! Great and very lucid explanation!
👌🏼
Ma’am / sir should not the diagram have high aldosterone levels on the side which depicts prolonged diuretic dosage ?
Excelente resumen
Nice, i agree with the post.
Very nicely explained. Thank u