Lama Ghazi, MD PhD
Postdoctoral Associate at Clinical and Translational Research Accelerator, Yale University School of Medicine
@lama_ghazi
I always want to know how the story ends as soon as I start and I always prefer when people lead with a summary before their talks. So, that is what I’ll be doing here.
Some patients when they get “sick”, they load up on multivitamins, herbs, teas and other home remedies. This is not what this blog is about. This is about whether we should advise patients to hold their antihypertensive medications when “sick” and restart them when feeling better to prevent acute kidney injury (AKI).
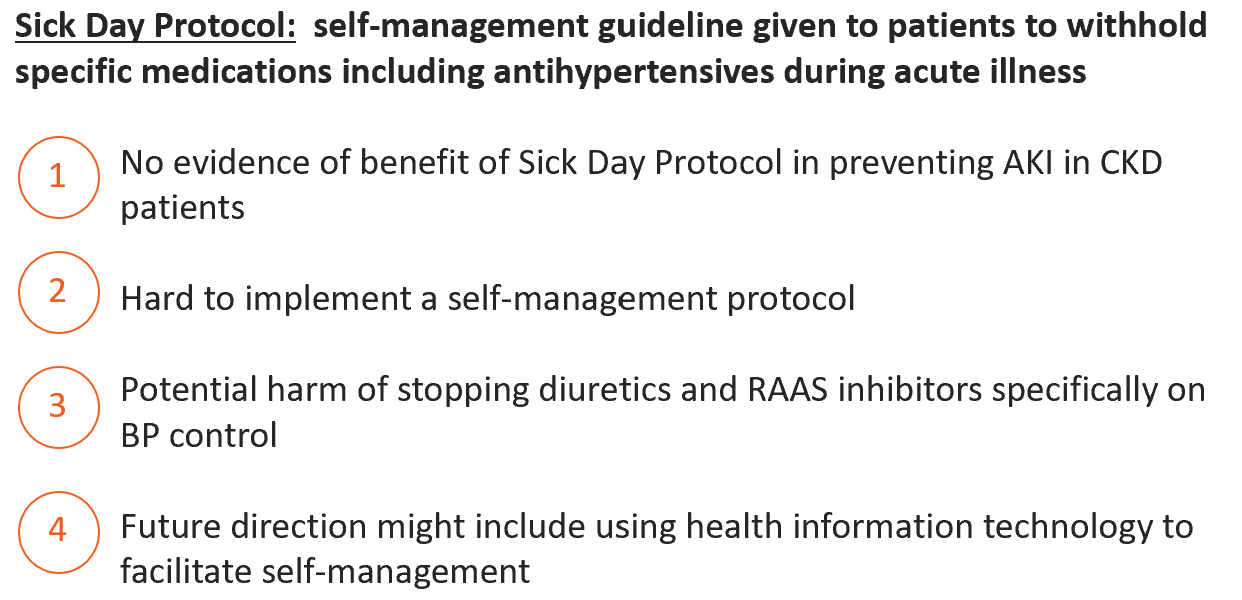
To sum up the whole discussion, look no further:
And now back to the beginning, we all know that AKI is a significant risk factor of chronic kidney disease (CKD) and is more prevalent in patients with CKD(Kidney inter., Suppl. 2012; 2: 1–138). Even mild and reversible AKI is associated with an increased risk of death (Kidney inter., Suppl. 2012; 2: 1–138). AKI is associated with progression of CKD, cardiovascular events and functional impairment (James, Nat Rev Nephrol, 2020). Additionally, patients with CKD are at a high risk of complications from AKI especially during acute illness (Kidney inter., Suppl. 2012; 2: 1–138).
Not only is AKI associated with significant morbidity and mortality, but AKI is associated with increased healthcare costs as well. In 2017, cost in the US was between $5.4 and $24 billion. In-hospital,AKI requiring dialysis increased the cost per hospitalization per patient by $40,000 (Silver, Nephron, 2017). In Canada in 2015, AKI-related healthcare costs were $140 million/year (Collister, Clin J Am Soc Nephrol, 2017/). Moreover, the progression from AKI to CKD leads to comorbidity development and to a further medical expense rise.
In order to prevent AKI and improve safety and outcomes, recommendations to temporarily stop “nephrotoxic” medications through self-management strategies during episodes of acute illness were considered to reduce AKI incidence in the community.
This was the beginning of Sick Day Rules i.e. resources to support medication self management during acute illness. This initiative was first institutionalized by the National Health Services Highland (NHS) in Scotland and is gaining momentum now in, UK and Canada (Scottish Patient Safety Programme; Think Kidneys NHS).
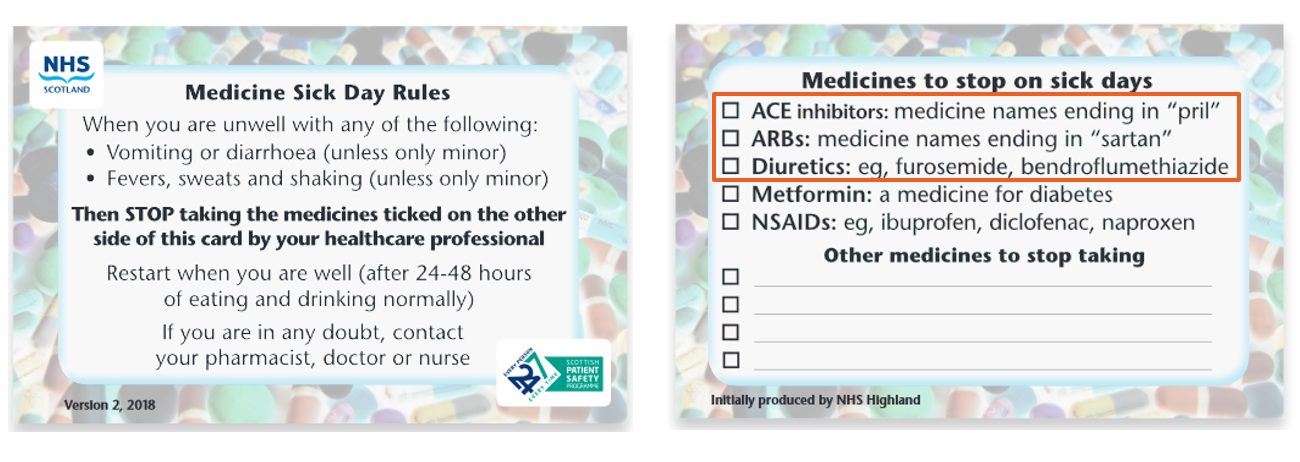
This is an example of a Sick Day Rules Card by the NHS Highland in Scotland. Most of the medications affect autoregulation of the kidney to include antihypertensive medications (angiotensin converting enzyme inhibitors [ACEi], angiotensin receptor blockers [ARB], diuretics). Non-steroidal anti-inflammatory (NSAIDS) can result in kidney injury in certain patient populations or medical conditions (it prostaglandin dependent renal perfusion).
The Canadian Diabetes Association Clinical Practice Guidelines for Type 2 Diabetes has a sick day protocol to prevent AKI (Canadian Diabetes Association, Sick Day Medication List, 2018). Patients are given a handout that recommends to pause certain medications using the acronym SADMANS if patients get sick: sulfonylurea, ACEi, diuretics/direct renin inhibitor, ARB, metformin, NSAID, and sodium-glucose cotransporter-2 inhibitors [SGLT2i]). If diuretics are prescribed in patients with heart failure, they recommend contacting their healthcare providers. Sickness is defined here as throwing up, having diarrhea ,a fever, or oral intolerance which can lead to dehydration. Patients are to restart their medications after they have recovered. In case they do not feel better or have questions, they are to contact their providers.
While many continue to teach sick day rules, no formal sick day guidelines exist in the United States (US) for patients with diabetes, hypertension, or CKD. However, the Sick Day Protocol for patients with type 1 diabetes to avoid diabetic ketoacidosis issued by the American Family Physicians, American Diabetes Association, and the CDC instructs patients to continue taking their insulin and diabetes pills as usual (Smith, Am Fam Physician, 2018; CDC Managing Sick Days, American Diabetes Association – Preparing for Sick Days).
As you may notice, certain antihypertensives and diuretics can lead to AKI if a patient is sick .
1) Diuretics help with blood pressure control and natriuresis. However, diuretics can increase the risk of AKI in patients with congestive heart failure, ascites, or edematous states especially if superimposed with volume depletion (Brater, N Engl J Med, 1998). Diuretics can also cause electrolyte disturbances (hypokalemia, hypomagnesemia, hypochloremia, metabolic alkalosis) (Palmer, Seminars in Nephrology, 2011).
2) Renin-angiotensin aldosterone system inhibitors (RAASi), which include ACEi and ARBs slow the progression of CKD and also reduce blood pressure (Gaudreault-Tremblay, Clin J Am Soc Nephrol, 2020). RAASi also increase AKI risk in the setting of volume depletion and this effect is enhanced if they are on on diuretics, SGLT2i, and NSAIDs by causing hypovolemia, afferent arteriole vasoconstriction, reduced intraglomerular pressure, and inhibiting prostacyclin synthesis leading to renal afferent arteriolar vasoconstriction respectively. (Gaudreault-Tremblay, Clin J Am Soc Nephrol, 2020;Lapi, BMJ, 2013 ;Hahn, Nat Rev Nephrol , 2016;Palevsky , Clin J Am Soc Nephrol , 2016).
What is the evidence behind stopping medications to prevent AKI? In short, not much, and not strong evidence. I will try to be brief and to the point. I struggled reading through all the Lord of the Rings Trilogy with all the descriptions and songs (not hating on J.R.R. Tolkien though) and I do not want you to struggle through this too.
We can always go back and discuss the literature in a separate post! Maybe I should go back and reread the Lord of the Rings after all, older and wiser me might like detailed descriptions. References are listed here for those who appreciate something more than a summary.
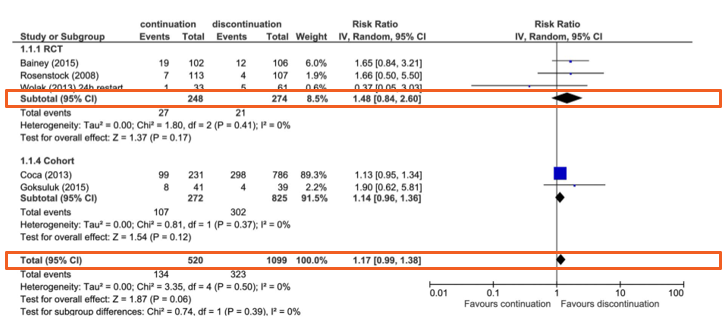
- A systematic review of 3 randomized controlled trials [RCT] and 3 cohort Studiesthat examined the effect of temporary discontinuation of ACEi/ARBs, direct renin inhibitors, NSAIDs, metformin, or sulfonylurea in patients with intercurrent illness or a radiological/surgical procedure, on AKI risk. There was ~15% increased risk of AKI in whom medication was continued compared with those in whom it was discontinued (relative risk [RR] 1.17, 95% confidence interval [CI] 0.99 to 1.38). When only results from RCTs were pooled, the risk increased almost upto 50% (RR 1.48, 95% CI 0.84 to 2.60), but the CI was much wider (Whiting, BMJ Open, 2016).
2. Using longitudinal electronic health record data, patients who were newly prescribed RAASi or diuretics compared to those who weren’t, had a higher risk of AKI (hazard rate: 1.23 [1.04, 1.45]), however the absolute increased of AKI was low (absolute risk of AKI in patients prescribed RAASi or diuretics: 25 events/1000 PY) and limited to patients who were prescribed both RAASi and diuretics. The magnitude of benefit (prevention of ischemic heart disease, cerebrovascular disease, CKD, ESKD, all-cause and cardiovascular mortality) of RAASi and diuretics, however, outweigh the risk (Scott, BMC Nephrology, 2019).
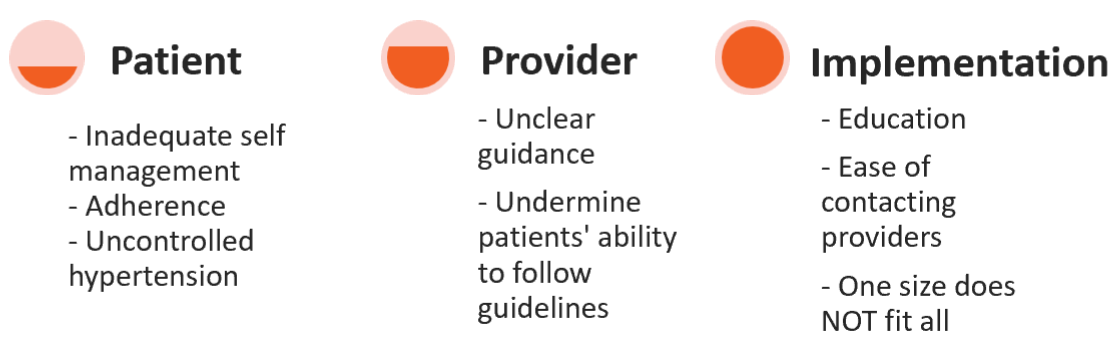
Has the sick day protocol been implemented? YES, but with frustrations! The sick day protocol was implemented in the primary setting across England between 2015-2016 and included 29 providers. Providers found that the concept of sick-day protocol was not straightforward or easy to understand, guidance should be explained in person, the response to guidance is subjective and it was difficult to implement (Morris, BMC Family Practice, 2016; Martindale, BMJ Open, 2017).
At the University of Maryland in Baltimore, they tested the usability of the sick day protocol in 20 patients with CKD stage 3-5 and found that there was a striking failure to identify correct medications to withhold and that the efficacy of the protocol is still to be determined (Doerfler, Clin J Am Soc Nephrol, 2019).
PROS of sick day protocol: discontinuing diuretics and RAASi might prevent AKI
CONS of sick day protocol: table….
There are ongoing studies examining these protocols, for example, an upcoming clinical trial on Sick Day Protocol to Improve Outcomes in Chronic Kidney Disease (ClinicalTrials.gov Identifier: NCT03141905) to be completed July 2022.
To top it all off, here are my recommendations:
- Not enough evidence supporting the use of Sick Day Protocol in patients with CKD to prevent AKI
- More harm can be done by temporarily discontinuing ACEi/ARB and diuretics
- Relying on patients to make clinical decisions is complex and further studies are needed
In order to assess if a sick day protocol results in meaningful reduction of AKI, we need:
- RCT to test whether withdrawal of ACEi/ARB or diuretics prevent adverse events during acute illness
- Assess if “nephrotoxic” medication dose changes prevent AKI in patients with CKD during acute illness (Perazella, Clin J Am Soc Nephrol, 2018)
- Weigh the risk-benefit of temporary stopping ACEi/ARB or diuretics in patients with certain comorbidities
- Design and test reliable self-management interventions to reduce drug associated AKI
- Test if health information systems can be leveraged to prevent AKI during sick days
- Maybe you can tackle these in your next grant or study! Please make sure to mention the great influence I had!
Reviewed by Sudha Mannemuddhu @drM_sudha, Mathew Sparks @Nephro_Sparks, Amy Yau @amyaimei, Anju Yadav @docanjuyadav

A very nice summary of the relationship between AKI and CKD! Thank you!
You mentioned that some “nephrotoxic” medications might affect autoregulation of the kidney which might be associated with AKI if my interpretation is correct. Do you know if there are any clinical studies looking at the contribution of kidney autoregulation in AKI or to CKD progression?