Brian Rifkin, MD
Interventional and General Nephrology Hattiesburg Clinic
Hattiesburg, MS
@brian_rifkin
The push to have more patients dialyzed in the home setting is gaining momentum in the United States (US) under programs like the ETC (ESRD Treatment Choices), in which some nephrology practices were mandatorily enrolled in 2021. The ETC is specifically designed to incentivise nephrologists to increase the number of patients utilizing home dialysis and increase the number of patients on the kidney transplant waiting list.
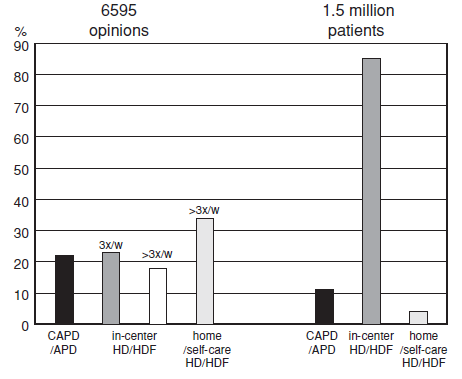
Starting a patient on a home dialysis modality is a reasonable goal in many circumstances. Past surveys suggest a majority of healthcare professionals would choose a home dialysis option if they themselves required kidney replacement therapy and transplantation was not an immediate option (Figure 1). Unfortunately, there are many reasons patients are unable to stay home for dialysis. Let’s examine some of the medical reasons behind patients’ plans for home dialysis ending prematurely.
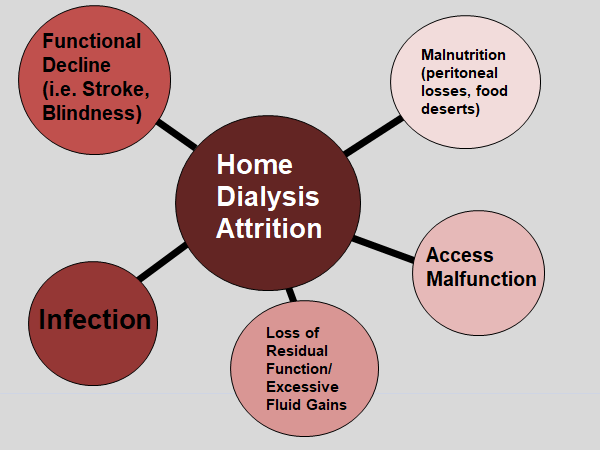
The first few months after initiation have the highest associated risk of leaving home dialysis, most commonly due to infection or dialysis access dysfunction. Patients on home hemodialysis (HHD) and peritoneal dialysis (PD) may suffer from loss of residual kidney function, inadequate clearance, malnutrition, and decline in functional status that requires a switch to in-center dialysis (Figure 2).
Training/Education: Lack of familiarity or bias can lead patients to not being considered for HHD, or being transferred to in-center HD prematurely if the physician/care team is uncomfortable managing complications.
- Low physician comfort/familiarity: In Hong Kong where PD is a required first line therapy, two year technique survival is 82% (versus 68% in the US, see Figure 3). Large numbers of patients initiating PD equates to increased staff expertise, physician comfort with complications, and shorter training times (only 4-5 days on average). Many nephrologists in Hong Kong are trained in the placement and maintenance of PD catheters as well, decreasing delays seen when referring to a surgery clinic. By contrast, a sheer lack of exposure in the US may account for significant physician discomfort with PD. In a survey of nephrology training programs only 32% of nephrology fellows reported attending outpatient PD clinics. Among those with PD clinic exposure, US nephrology fellowship programs reported only 30% had more than 5 patients per trainee (Chaudhary K. Int J Nephrol, 2011).
- Lack of appropriate patient education: In addition to physician issues, patient centered training issues also account for the diminished number of patients choosing home dialysis modalities . Higher rates of early failure were seen in patients with lower literacy scores, those without a partner and patients who were unemployed.
- Staff training/familiarity: Finally, having adequate nursing and support staff who are confident in their skills and teaching abilities are compulsory to any home program. You can’t build an efficient program without the right personnel.

Ultrafiltration: Ultrafiltration failure is a significant complication that may require a dialysis modality change. A functioning peritoneal membrane has characteristics that make the removal of water and uremic solutes possible. Complications of ultrafiltration loss can be worsened by loss of residual kidney function or excessive fluid intake. Proteins embedded within the peritoneal membrane have specific transportation characteristics. For example, Aquaporin-1 (AQ1) is expressed in the endothelial cells lining the peritoneal capillaries. High dose intravenous dexamethasone has been shown to increase AQ1 expression and enhance ultrafiltration in animal models. Medication enhanced transport of fluid could potentially be used to augment ultrafiltration and prolong PD viability (Mehrohta R, et al. JASN, 2016) .
Peritoneal inflammation can negatively impact the peritoneal membrane. Advanced glycosylation products from routine use of high dextrose containing solutions may worsen inflammation and alter membrane solute transport characteristics. Biocompatible solutions (i.e. icodextrin) have been shown to effectively decrease fibrosis in mice (Cuenca M, et al.Int Urol Nephrol, 2018). Biocompatible PD solutions are characterized by a neutral pH and low glucose degradation product concentrations. However, the published evidence in humans supporting their use has often been conflicting and of variable methodological quality (Htay H, et al. Cochrane Database Syst Rev, 2018). Lastly, maintaining volume homeostasis is dependent on residual kidney function. Residual kidney function directly affects mortality and with an increase of just 250 ml of urine volume per day there was an associated 36% lower 2-year mortality in dialysis patients. Further development of pharmacologic treatments and improved biocompatible solutions may help to preserve and even positively alter the peritoneal membrane, prolonging its duration of usefulness.
Peritonitis: Both physicians and patients are often concerned about the risks for infection. Rates of peritonitis have declined in recent years due to training, twin bag systems and antimicrobial prophylaxis protocols (including use of antifungals and mupirocin for nasal colonization of Staphylococcus). Additionally, daily catheter care checklists used before and during exchanges have assisted in decreasing infection rates. Peritonitis occurs roughly once every eighteen months on average and peritonitis relapses in 3-20% of cases resulting in catheter removal in 22% and death in 2-6%. Most peritoneal infections are not as severe as those seen in hemodialysis patients with bacteremia. Patients are routinely treated at home unless there are signs of severe sepsis or extreme pain or nausea. Unfortunately, even after treatment of an acute peritonitis episode, the risk of death from infection, cardiovascular disease and withdrawal from home dialysis remains elevated for up to 6 months.
Of note, Peritonitis treatment often requires gram positive and gram negative coverage with intraperitoneal preferred over intravenous(IV) and oral (PO) routes. Treatment guidelines are beyond the scope of this discussion but can be found at ISPD.org. In addition to antibiotics, pain control, intraperitoneal heparin for fibrin, fungal prophylaxis as well as technique review and re-education are the cornerstones of treatment.
Dialysis Catheter Dysfunction: Finally, mechanical catheter issues may lead to the need to transition off peritoneal dialysis for prolonged periods. PD catheters may be slow to fill or drain or may have associated discomfort during exchanges (Shah A. RFN, 2018). Migration, blockage due to omental trapping and fibrin clogging are just a few of the possible complications. There are strategies to try to limit impaired catheter flow. Use of laxatives and frequent bladder emptying may help in prevention of catheter tip obstruction. Use of heparin or tPA can be used in the clinic for relieving fibrin plugs. Timely surgical correction by catheter manipulation, omentopexy, lysis of adhesions and colpopexy may help to salvage a defective catheter (Yilmazlar T, et al. Perit Dial Int, 2006).
Telehealth: Telehealth, which became much more widely used in 2020, may play a key role in decreasing home dialysis attrition. More frequent data points (blood pressure, weight, ultrafiltration data) may help physicians and nurses catch critical treatment issues sooner. More frequent adjustments in patient prescriptions may prevent rapid declines that result in hospitalizations (Weinhandl E. Hemodial Int, 2018). More connectivity with home dialysis patients will allow for timely responses to shortened or missed sessions, and course corrections. Regular communication through telehealth will hopefully allow problems to be addressed earlier and more thoroughly.
Home Hemodialysis: Although peritoneal dialysis has been the primary home modality in the last two decades, other home modalities are gaining momentum. Home hemodialysis (HHD) currently accounts for 3.5% of incident dialysis patients in the US (versus PD at approximately 10%). Both HHD and PD are showing steady growth over the last decade. Compared with PD, patients using HHD have a 20% lower mortality and 30% lower technique failure, but these results may represent selection bias (Yu J, et al. Semin Dial, 2018). HHD has shown advantage in observational studies and has been associated with higher quality of life, decreased depression, and decreased post dialysis recovery time. Still, HHD is not widely employed due to reimbursement issues, lack of physician familiarity, and insufficient numbers of trained personnel (Jayanti A, et al. Hemodial Int, 2014).
HHD attrition, similar to PD, may be due to transplant, death, technique failure, access loss, and conversion to in-center HD. Most complications are due to vascular access problems, infection related hospitalization and patient fatigue. There have been few randomized controlled trials examining the differences between HHD and conventional in-center hemodialysis (Ramakrishnan, M. RFN, 2019). Thus, there isn’t currently a body of evidence to conclusively say that HHD is a better form of kidney replacement therapy than either conventional in-center HD or PD.
Being home and staying home should be the goal for patients with kidney failure. Although there are many reasons why a patient may not be able to accomplish home dialysis treatments, increased support through telehealth and further education and training of patients and physicians will help greatly expand home dialysis options in the US. Unfortunately, complications of dialysis are common among all patients on kidney replacement therapy. Further refinement of protocols and procedures will hopefully make patients feel safe at home. Finally, further research is needed to understand the barriers to initiation of home dialysis, and what additional care can be offered to support patients at home.
Reviewed by Matthew A. Sparks, MD and Amy Yau, MD

