Welcome to the 20th case of the Skeleton Key Group, a team of 50-odd nephrology fellows who work together to build a monthly education package for the Renal Fellow Network. The cases are actual cases (without patient identifying information) that intrigued the treating fellow.
Written by: Bilal Sheikh
Visual Abstract & Infographics: Mythri Shankar & Krithika Mohan
A. The Stem
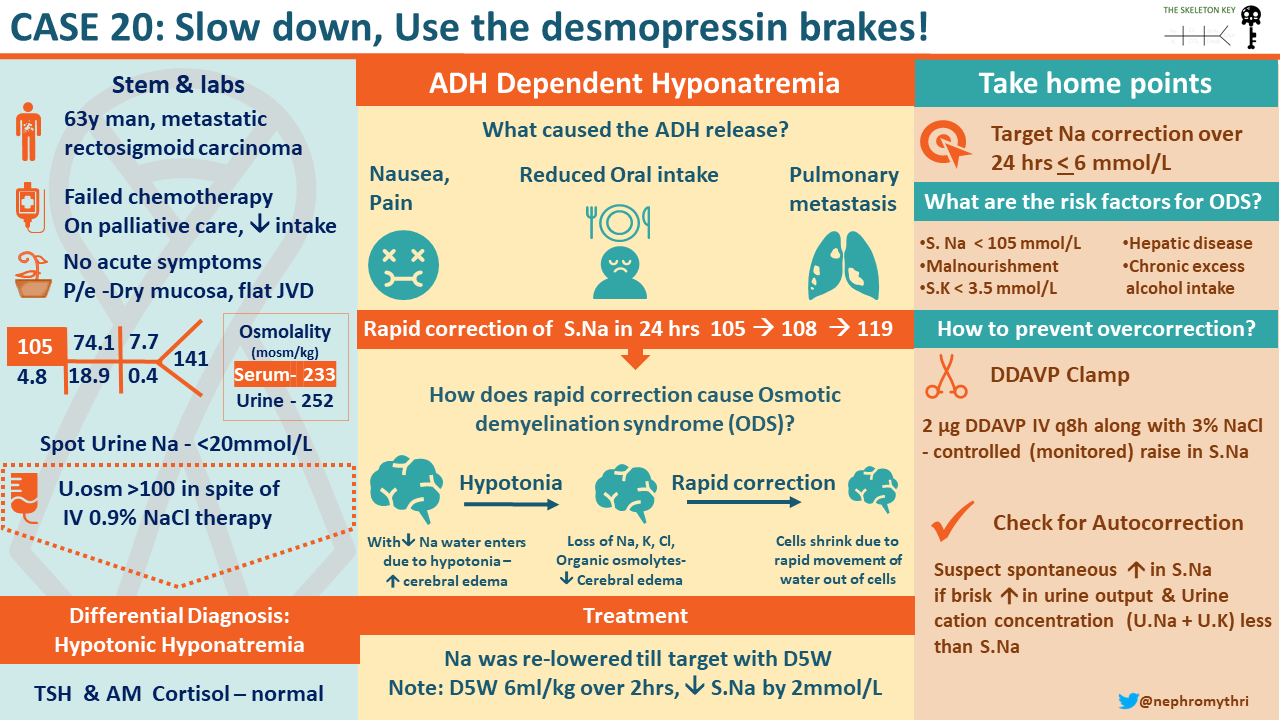
A 63-year-old man diagnosed with rectosigmoid cancer with hepatic and pulmonary metastases presented to the emergency room with nausea for the last few days, not improved with ondansetron. He has not been able to take anything by mouth. He denied vomiting, constipation or abdominal pain. On review of systems, he had fatigue and malaise. He was diagnosed with rectosigmoid cancer 2 years prior, but cancer has failed to respond to multiple chemotherapy treatments. He is currently on supportive palliative care but is not receiving any palliative chemotherapy.
He also had diabetes mellitus, hypertension and coronary artery disease. He is not a smoker and he denies any history of alcohol or recreational drug use. His medication list includes aspirin, clopidogrel, tramadol, acetaminophen, omeprazole, amlodipine, carvedilol, and insulin.
Vital signs:
BP 115/75 mm Hg, HR 95 bpm, RR 16/minute, SpO2 98% without supplemental oxygen, Temp: 36.5 °C (97.7 °F), Weight 77 kg
Physical examination:
Physical examination revealed a thin man, alert and oriented, but slow to respond; mucous membranes appeared dry and he had flat jugular venous distension. The rest of the exam was unremarkable.
He was initially given intravenous omeprazole and ondansetron along with IV 0.9% normal saline.
B. The Labs:
The most recent labs available for comparison were from 18 days before presentation, showing a serum sodium level of 127 meq/L.
C. Classification of hyponatremia
We see hyponatremia on the chemistry panel. Let’s discuss how hyponatremia can be classified: this helps to guide us in determining the work up and appropriate management options for the patient.
Hyponatremia is classified based on severity, duration, presence (or absence) of symptoms, and serum osmolality.
- Severity – based on serum sodium levels; between 130 and 134 is mild, between 125 and 129 is moderate, while less than 125 is considered severe.
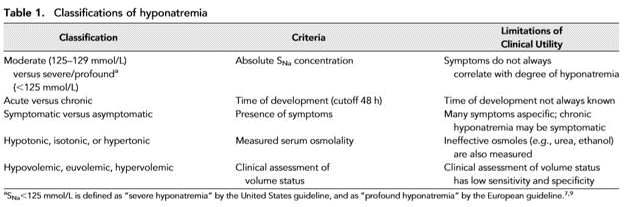
Acute vs Chronic – if hyponatremia has been present for less than 48 hours, it is considered acute, while hyponatremia for a duration greater than 48 hours is classified as chronic hyponatremia. Now, this is tricky; when a patient presents with hyponatremia, usually we don’t have values of serum sodium for the past 24- 48 hours. Usually in such cases when the exact duration is unknown, hyponatremia is considered chronic.
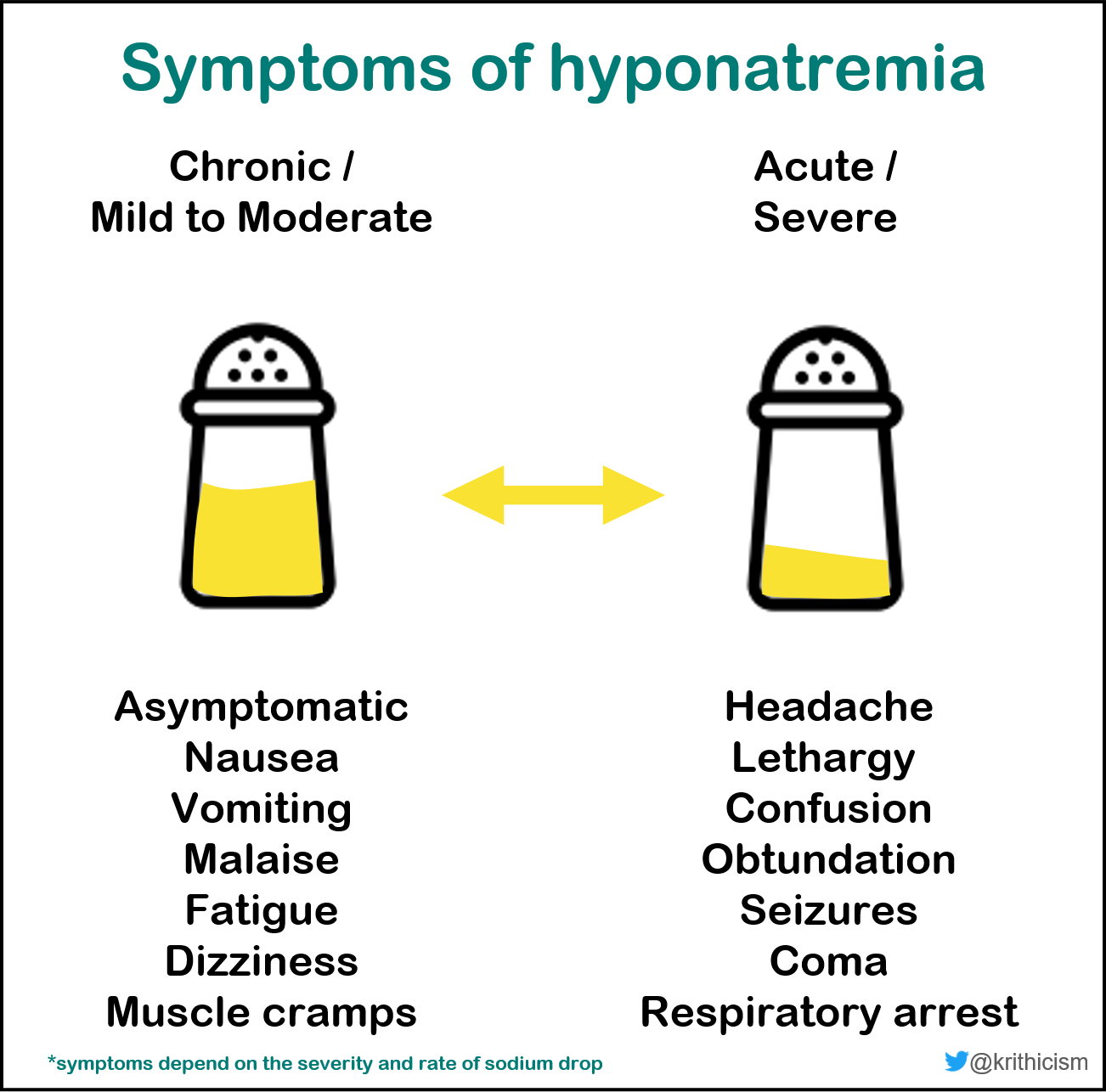
- Symptoms – symptoms of hyponatremia are related to disturbances of the central nervous system. They include fatigue and nausea, gait disturbance, memory problems, and lethargy. Severe symptoms like seizures and coma, can occur as well. Symptom development depends on the acuity and severity of serum sodium change: the more rapid the onset and the more severe the degree of hyponatremia, the worse the symptoms. That is because slower changes in sodium concentrations allow for the time to adapt.
- Hypoosmolar vs non-hypoosmolar – the normal serum osmolality is 275-295 mOsm/kg; based on serum osmolality, the hyponatremia can be categorized as hypoosmolar or non-hypoosmolar.
Diagnostic algorithm/Initial workup
The diagnostic workup of hyponatremia can be really daunting. A commonly used algorithm is found below:
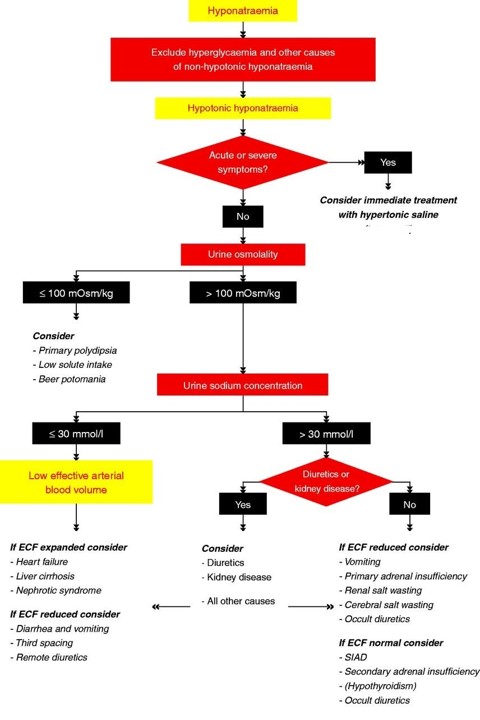
Therefore, the first test we usually order is serum osmolality to determine if it is hypoosmolar hyponatremia or non-hypoosmolar hyponatremia. For a discussion on non-hypoosmolar hyponatremia, please check out this SKG case from Jefferson Triozzi.
Remember that hyponatremia is a problem of excess free water, so once we know we are dealing with hypoosmolar hyponatremia (aka true hyponatremia), we need to know if the kidneys are doing their job of excreting excess free water. Urine osmolality helps us in evaluating that. We use a cut-off of 100 mOsm/kg; above this threshold there is antidiuretic hormone (ADH) present which is the culprit for retention of free water. One exception is acute kidney injury or chronic kidney disease, when kidneys cannot maximally dilute the urine to get rid of excess free water.
- More Data:
Additional lab results are shown below:
| Serum osmolality (mOsm/kg) | 233 |
| Urine osmolality (mOsm/kg) | 252 |
| Urine Na+ (mmol/L) | < 20 |
- Diagnosis:
It should be emphasized that a good history and careful review of medications, help clinicians narrow down the differentials. As an example, history of fluid-loss from vomiting or diarrhea points towards hypovolemia, while presence of malignancy, or CNS or pulmonary disease, gives a clue to possible SIADH. In addition, the list of medications that can cause SIADH is never ending, but famously include drugs acting on CNS (antiepileptics, antidepressants, antipsychotics), chemotherapeutic agents, amiodarone among others. Finding out if the patient is taking any of those will be an important clue to SIADH.
Before we discuss our diagnostic approach, let’s spend some time on the utility of the diagnostic tests that we are ordering.
- Urine Osmolality: The dichotomy starts with urine osmolality, with a cutoff of ≤100 mOsm/kg. Regardless of the specific number, low urine osmolality reflects the absence of ADH, while high urine osmolality indicates its presence.
The differential for hyponatremia with a urine osmolality less than 100 mOsm/kg is pretty narrow and consists of: i) primary polydipsia, ii) low dietary solute intake. In our case the urine osmolality was 252, thus making these possibilities less likely.
A higher urine osmolality (> 100 mOsm/kg) in the presence of hyponatremia signifies the presence of ADH. Next we have to determine if the ADH release is appropriate or inappropriate. Hypovolemia and hypertonicity are the 2 appropriate stimuli for release of ADH: ADH is released to correct hypovolemia or hypertonicity in these scenarios respectively. ADH is also released when effective arterial circulatory volume is low (despite the high extracellular volume) as is the case in heart failure, liver failure or nephrotic syndrome. An inappropriate release of ADH, independent of volume or tonicity stimuli, can occur due to a number of factors, including nausea/vomiting, medications, paraneoplastic syndromes etc.
This is accomplished in a few simple steps, utilizing physical examination, in conjunction with urine sodium concentration.
Unfortunately, clinical assessment is an unreliable tool to determine volume status in hyponatremic patients. For practical purposes, during the evaluation of hyponatremia, we consider a patient euvolemic unless they are grossly volume depleted or overloaded. Once we have this information, we can classify it into 4 scenarios:
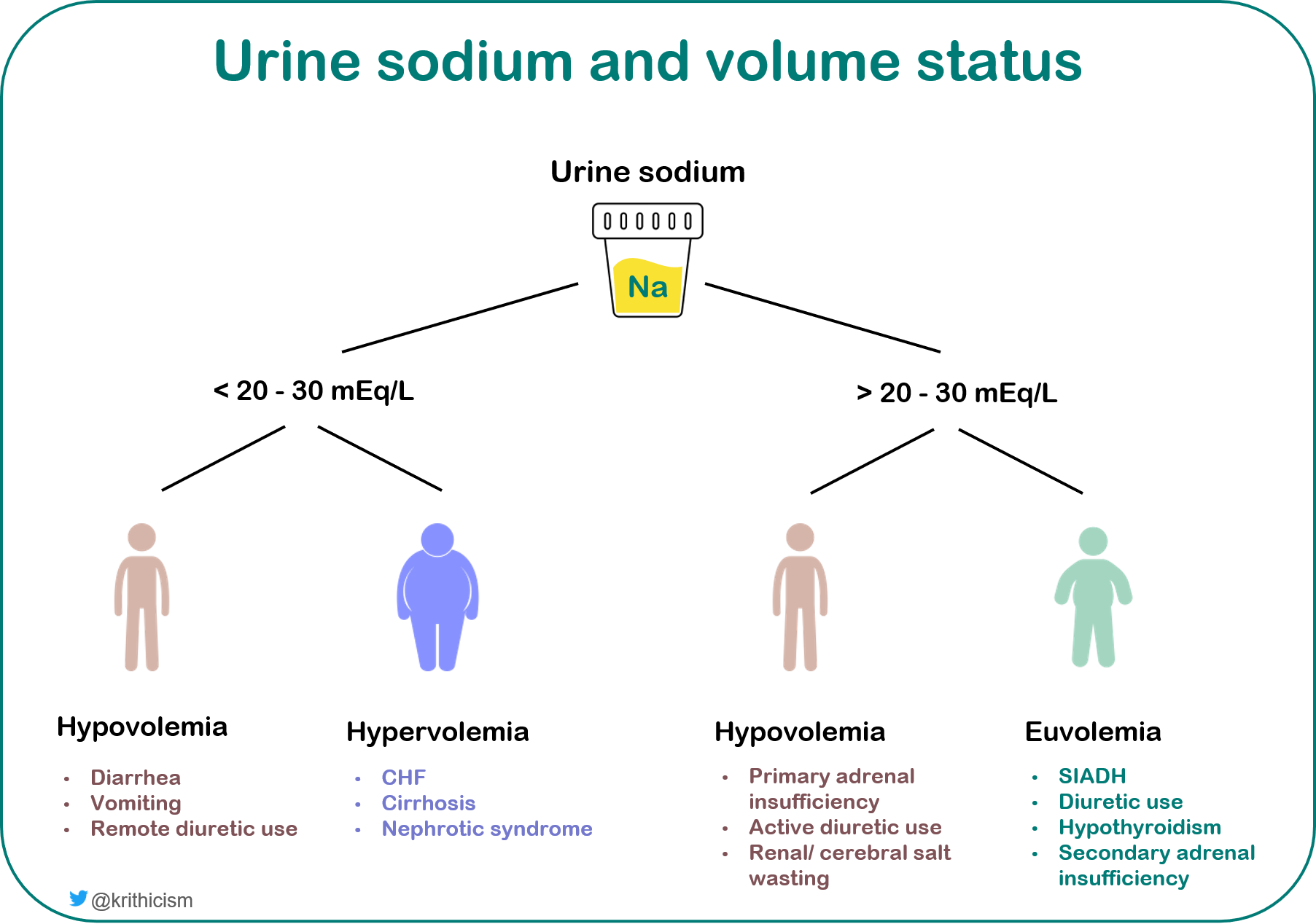
It should be emphasized that these buckets should not be considered mutually exclusive, and in a given patient, there may be more than one mechanism contributing to development of hyponatremia.
Applying that to the case:
The sodium level is dangerously low and is classified as severe hyponatremia. Based on the available data, we cannot reliably say if development of hyponatremia was really acute (no labs on the preceding 24-48 hours); therefore, the safest bet is to treat it as a chronic problem. Another clue that speaks in favor of this being a chronic issue are his mild symptoms. Acute drops in sodium would almost always make a patient more symptomatic. Random finger stick blood glucose rules out hyperglycemia causing pseudohyponatremia, which is also supported by low serum osmolality. So, we are dealing with a true hyponatremia.
Hypo-osmolar hyponatremia in this patient with cancer has a lengthy differential:
- The history of decreased oral intake along with physical exam findings of hypovolemia support hypovolemia as a cause for hyponatremia
- Nausea itself is also a potent stimulus for ADH.
- On the other hand, he was not receiving any chemotherapy which rules that out as a cause for SIADH, but his medication list includes tramadol which can independently cause SIADH. History of pulmonary metastatic disease also favors the diagnosis of SIADH.
Our differential is supported by the laboratory evaluation as well: his urine osmolality was high (> 100) which means we are looking at an ADH-dependent phenomenon. Urine sodium less than 20 mmol/L supports hypovolemia as a major contributor to the release of ADH.
D. Management
Management of chronic hyponatremia is aimed at correcting serum sodium to relieve the symptoms while avoiding any harmful effects. This begins with identification of reversible causes of hyponatremia, review of medications that may cause inappropriate secretion of ADH, and reduction of electrolyte free water intake. In patients with chronic hyponatremia, a rate of correction of 6 mEq/L in any given 24-hour period is considered safe. In hyponatremic patients with hypovolemia, isotonic saline is used to replete volume. It is also recommended to initiate desmopressin (DDAVP), a synthetic ADH analogue, concomitantly to prevent rapid overcorrection (more on this below). With that, serum sodium should be checked serially to make sure it is correcting appropriately.
Considering hypovolemia to be the predominant contributor to hyponatremia, the patient was started on IV hydration with 0.9% normal saline. Since he was on palliative care, the family and the patient insisted that labs only be drawn when necessary. His sodium trend was below:
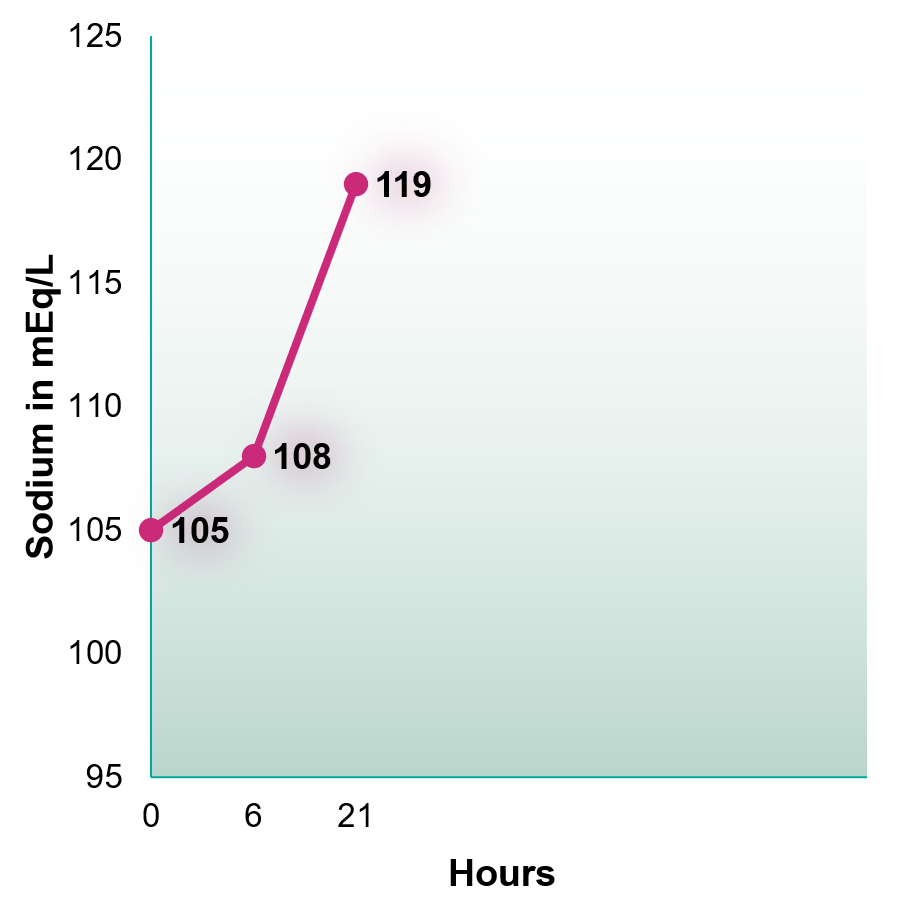
The serum sodium corrected by 14 mmol/L in less than 24 hours! Overly rapid correction can be seen in patients in whom a rapidly reversible stimulus of ADH is present and is reversed; in our patient, hypovolemia appears to be the particular cause. Other instances where rapid correction can occur include: cessation of exogenous DDAVP therapy, administration of exogenous cortisol (when adrenal insufficiency is the causing SIADH) or administration of hypertonic saline.
E. Dealing with the Complication
Overly rapid correction of hyponatremia can lead to irreversible brain damage. With hyponatremia and resultant loss of tonicity in the serum, water enters into the brain, resulting in cerebral edema. However, this is followed by loss of solutes and organic osmolytes resulting in restoration of brain volume relieving cerebral swelling. This process starts within hours and is completed over the next several days.
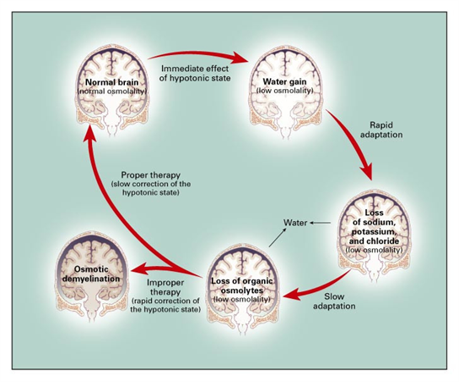
This adaptation by the brain, while helpful in avoiding cerebral damage due to hyponatremia, is the reason that overly rapid correction is not well-tolerated and may lead to neurologic complications, termed osmotic demyelination syndrome (ODS). If the serum sodium corrects rapidly, neurons start to shrink as the organic osmolytes, lost in the process of adaptation, cannot be replaced that quickly. Within hours, neurons, especially astrocytes and oligodendrocytes, begin to die leading to demyelination.
Risk factors for ODS include:
- Serum sodium < 105 mEq/L
- Hypokalemia
- Acute or chronic liver disease
- Chronic excess alcohol intake
- Malnourishment
Clinical manifestations of ODS and diagnosis:
The symptoms of ODS may be delayed for two to six days after rapid overcorrection, and include dysarthria, dysphagia, paraparesis or quadriparesis, behavioral disturbances, movement disorders, seizures, lethargy, confusion, obtundation and coma. The symptoms are usually irreversible.
Diagnosis is based on clinical history, clinical features and imaging findings of the central nervous system (CNS). MRI usually shows demyelination in the pontine and extrapontine regions of the brain, however the findings may be delayed in some cases for up to 4-6 weeks.
Prevention of ODS:
Because of the significant morbidity associated with ODS and lack of any treatment options, every attempt should be made to prevent rapid overcorrection of sodium. Sodium should be carefully monitored (at least every 4-6 hours) to avoid rapid overcorrection.
Prevention of ODS:
Because of the significant morbidity associated with ODS and lack of any treatment options, every attempt should be made to prevent rapid overcorrection of sodium. Sodium should be carefully monitored (at least every 4-6 hours) to avoid rapid overcorrection.
- Re-lowering the serum: If the serum sodium overcorrects, it should be re-lowered with the use of 5% dextrose in water (D5W) and desmopressin (DDAVP). D5W is given at a rate of 6 ml/kg over 2 hours; it lowers the serum sodium by approximately 2 mEq/L. The dose is repeated until the target serum sodium is achieved. Desmopressin is given at 2 mcg every 6 hours either intravenously or subcutaneously. Desmopressin is continued until sodium is in the safe range.
- DDAVP Clamp: this proactive strategy can be used to prevent rapid overcorrection. This includes inducing a state of iatrogenic SIADH by using desmopressin upfront with 2 mcg of desmopressin given every 6 hours either through intravenous or subcutaneous route, along with the use of 3% hypertonic saline bolus while the serum sodium is then raised gradually. This is recommended especially when hyponatremia is severe, or a rapidly reversible cause of excess ADH can be identified (e.g. hypovolemia, medication use, adrenal insufficiency etc). (More on this in our tweetorial by our very own Dr Kartik Kalra)
Wrapping the case up:
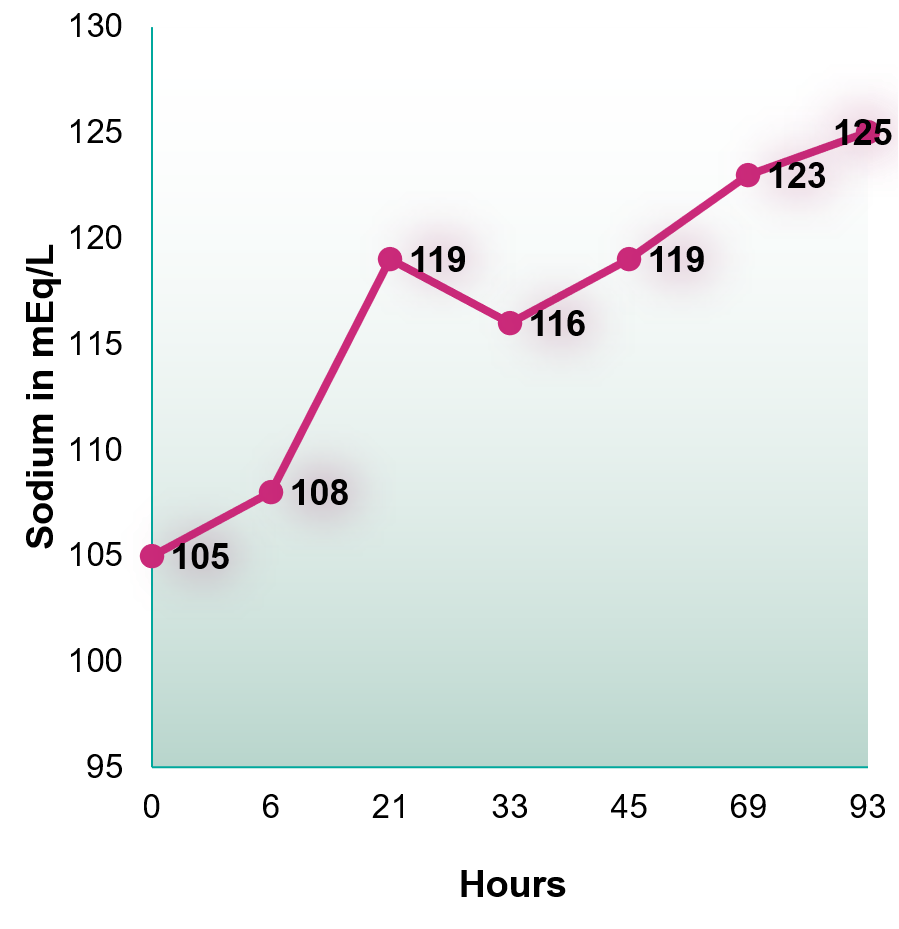
Saline was stopped, and the patient was given 600 ml of free water in the form of D5W infusion. Repeat sodium measurement was not obtained until 10 hours later which came back to 116 mmol/L. He was then started on IV 0.9% normal saline at 75 ml/hr while serum sodium was repeated over the next few hours which gradually corrected.
F Take Home Points
- The guidelines recommend rate of correction for hyponatremia of 10 mmol/L in any given 24-hour period: many clinicians are more conservative.
- Rapid serum sodium correction can cause ODSe and is associated with poor outcomes.
- In cases where serum sodium rapidly overcorrects, it should be relowered using 5% dextrose in water and DDAVP.
- Proactive strategy with DDAVP clamp be employed in cases where risk factors for rapid overcorrection can be identified.
Post Reviewed by Matt Sparks, Joel Topf, Anna Gaddy

Awesome. Thank you.