Urinary crystals are a frequent finding and there are several different types that can be observed under the microscope. We’ve discussed some of these crystals in a previous Urine Sediment of the Month post. Unlike these more common crystals that usually are not linked to diseases, pathologic crystals can be a link to relevant disorders. Here we will present you some useful information on these rare but relevant crystals.
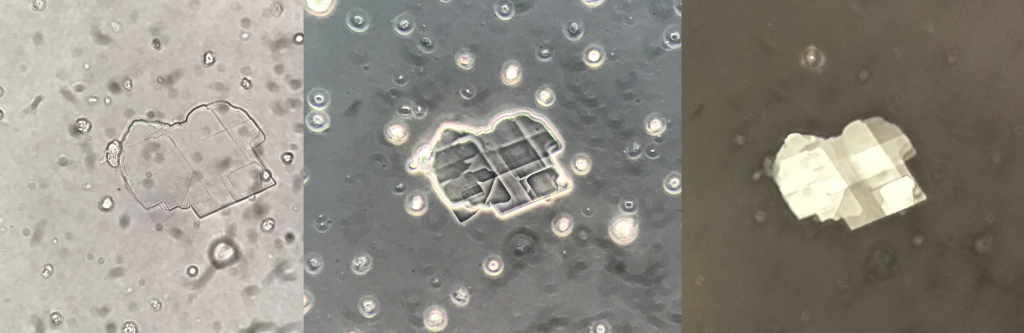
Cholesterol Crystals
Cholesterol crystals are thin, colourless and transparent plates with well-defined edges, which can be isolated or in aggregates, mostly seen in acidic urine. They are usually observed free in the urine sediment but can also be found within urinary casts [1]. They are associated with disorders producing lipiduria, such as the nephrotic syndrome, and are seen in conjunction with fatty casts and oval fat bodies. Cholesterol crystals are highly birefringent with polarized light and presents a monochromatic pattern using this type of microscopic filter [2].
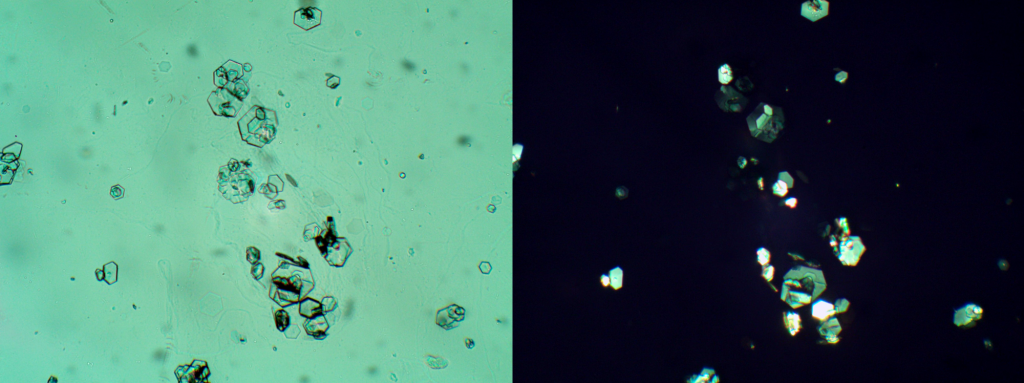
Cystine Crystals
Cystine crystals are thin hexagonal colourless plates with irregular sides. Occasionally, however, they may have a rosette-like appearance. They can be either isolated, heaped one upon another, or they may form aggregates. Under polarized light they are birrefringent presenting a monochromatic pattern [1]. It is important to mention that hexagonal crystals in urine are not exclusive to Cystine (despite the common belive says the opposite). Also uric acid and sulfamethoxazole [3] can precipitate as hexagons. A key point to differentiate between cystine and uric acid and sulfamothoxazole is the use of polarized light microscopy. Uric acid and sulfamethoxazole are polychromatic under polarized light, while cystine is monochromatic. Cystine crystals are typical of patients with cystinuria. This is a recessive inherited disease characterised by the deficient absorption, at renal tubular level, of cystine and dibasic amino acids lysine, arginine and ornithine. The consequences are urolithiasis and obstructive uropathy. The identification of typical crystals in the urine is a clue to diagnosis. The possibility to find cystine crystals in the urine is increased by acidic pH, since cystine has a high solubility at alkaline pH [1].
Bilirubin Crystals
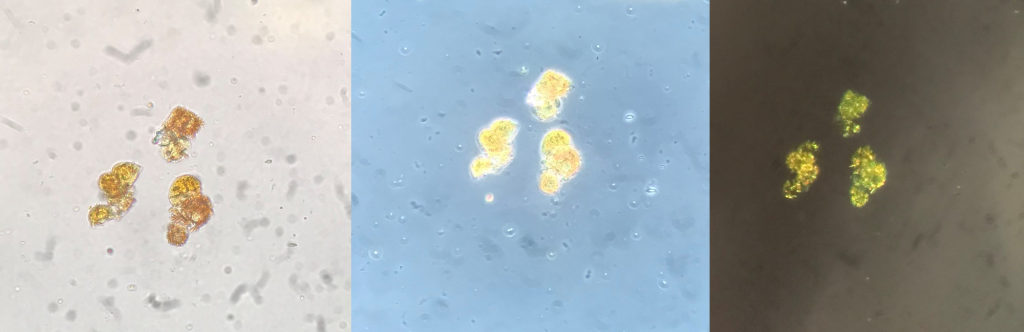
Bilirubin crystals are present in hepatic disorders producing large amounts of bilirubin in the urine. They appear as clumped needles or granules with the characteristic yellow color of bilirubin. They can be observed both, free and engulfed by white blood cells and renal tubular epithelial cells. Under polarized light they present a strong birrefringence being observed in patterns ranging from yellow to green. In disorders that produce renal tubular damage, such as viral hepatitis, bilirubin crystals may be found incorporated into the matrix of casts [2].

Leucine Crystals
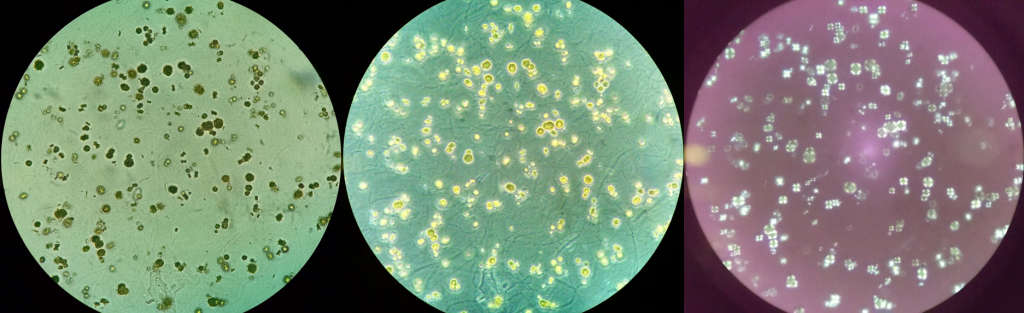
Leucine crystals appear as yellow-brown spheres resembling oil drops with concentric striations. Under polarized light, they form pseudo-Maltese crosses and presents a strong birrefringence with a yellow pattern. It is important to mention that calcium oxalate monohydrate (CaOxm) crystals can be stained by bile pigment and can present morphological resemblance with leucine.
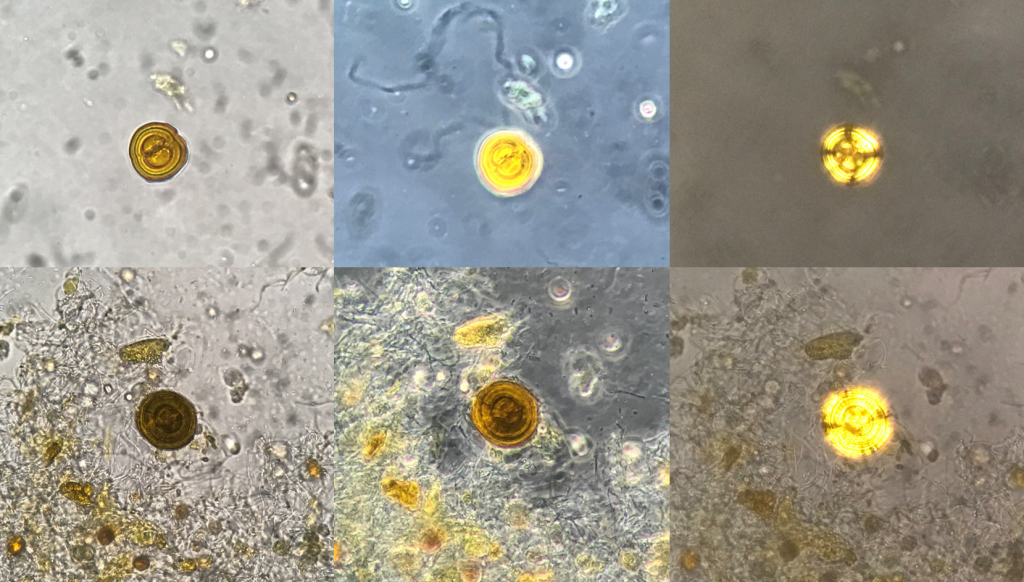
As mentioned earlier, polarized light is very usefull on crystals identification and can help in the differentiation between leucine crystals and CaOxm crystals because CaOxm crystals are polychromatic under polarized light (Figure 6) and leucine crystals are monochromatic (yellow) using this microscopic filter. The presence of leucine crystals is typical of patients with liver failure.
Tyrosine Crystals
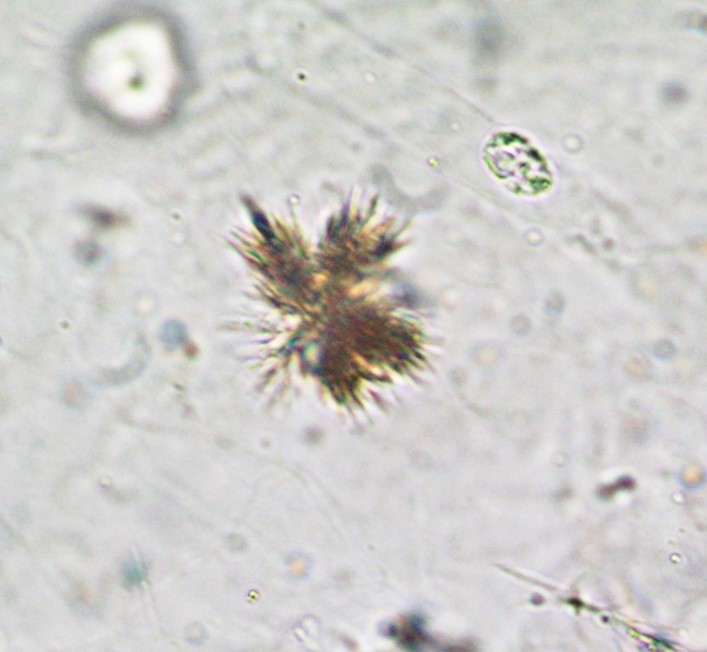
Tyrosine crystals appear as thin needles often aggregated in bundles or rosettes. Tyrosine crystals too are typical of patients with liver failure [1] and may also be encountered in inherited disorders of amino-acid metabolism [2].
2,8-dihydroxiadenine crystals
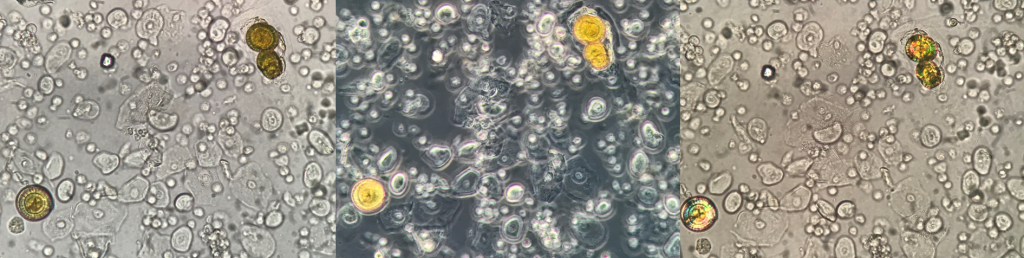
2,8-dihydroxyadenine (2,8-DHA) crystals are round and reddish-brown particles with a dark outline and central spicules, which under polarized light appear as “Maltese crosses”. However, especially in patients with severe renal function impairment, 2,8-DHA crystals may have atypical appearances with unusual birefringence features. 2,8-DHA crystals are found in the urine of patients with adenine phosphoribosyltransferase (APRT) deficiency, an enzyme which transforms adenine into adenosine monophosphate. Due to the enzyme deficiency, adenine is transformed by xanthine oxidase into 2,8-DHA, which is highly insoluble at any pH, a fact which is responsible for crystalluria [1].
Of note, these crystals were not identified by a confirmatory method, they are identified here as 2,8 dihydroxiadenine due to the morphological characteristics under the microscope.
Because of the rarity of these crystals it is extremely important that the professional performing urine microscopy to have the proper index of suspicion and resources to identify these abnormal findings.
Post by José Antonio Tesser Poloni
References:
- Fogazzi GB. The urinary sediment an integrated view. 3rd edition. Elsevier, 2010.
- Strasinger, Susan King. Urinalysis and body fluids/Susan King Strasinger, Marjorie Schaub Di Lorenzo; photography by Bo Wang [et al.]; illustrations by Sherman Bonomelli. — 5th ed.
- de Liso F, Garigali G, Ferraris Fusarini C, Daudon M, Fogazzi GB. How to identify sulfamethoxazole crystals in the urine. Clin Chim Acta. 2016 Jan 15;452:106-8. doi: 10.1016/j.cca.2015.11.006. Epub 2015 Nov 7. PMID: 26554520.