Paresh R. Jadav, MD (jadav_md)
Dept of Nephrology, Columbia University Medical Center, New York, NY
Introduction
Kidney allograft monitoring is dependent upon non-specific markers like creatinine, estimated glomerular filtration rate (eGFR), and proteinuria. Kidney biopsy remains the gold standard diagnosis for allograft dysfunction. The currently available, non-invasive markers are not sufficiently sensitive to detect early changes in allograft, while the pathological findings are often detected at relatively advanced stages. Early detection and treatment of subclinical events have been proposed to improve long term graft outcomes. Protocol biopsies are often performed to detect early pathologic changes prior to overt graft dysfunction via creatinine, eGFR, and/or proteinuria. However, biopsies are invasive, costly, labor intensive, and may incur complications; in addition, sampling errors could adversely affect its diagnostic use.
Management goals of transplant recipients entail maintaining a fine balance between suboptimal immunosuppression with its consequent rejection risks and over-immunosuppression with its adverse effects. Current diagnostic tools have fallen short in accomplishing these objectives. The rationale for seeking novel, non-invasive markers is to overcome the limitations of existing parameters in early diagnosis of graft dysfunction, achieving optimal immunosuppression, and long term surveillance of allograft function. Quantification of donor-derived cell free DNA (dd-cfDNA) is one such marker which has been proposed as a non-invasive tool to diagnose early allograft rejection.
Donor-derived cell-free DNA (dd-cfDNA)
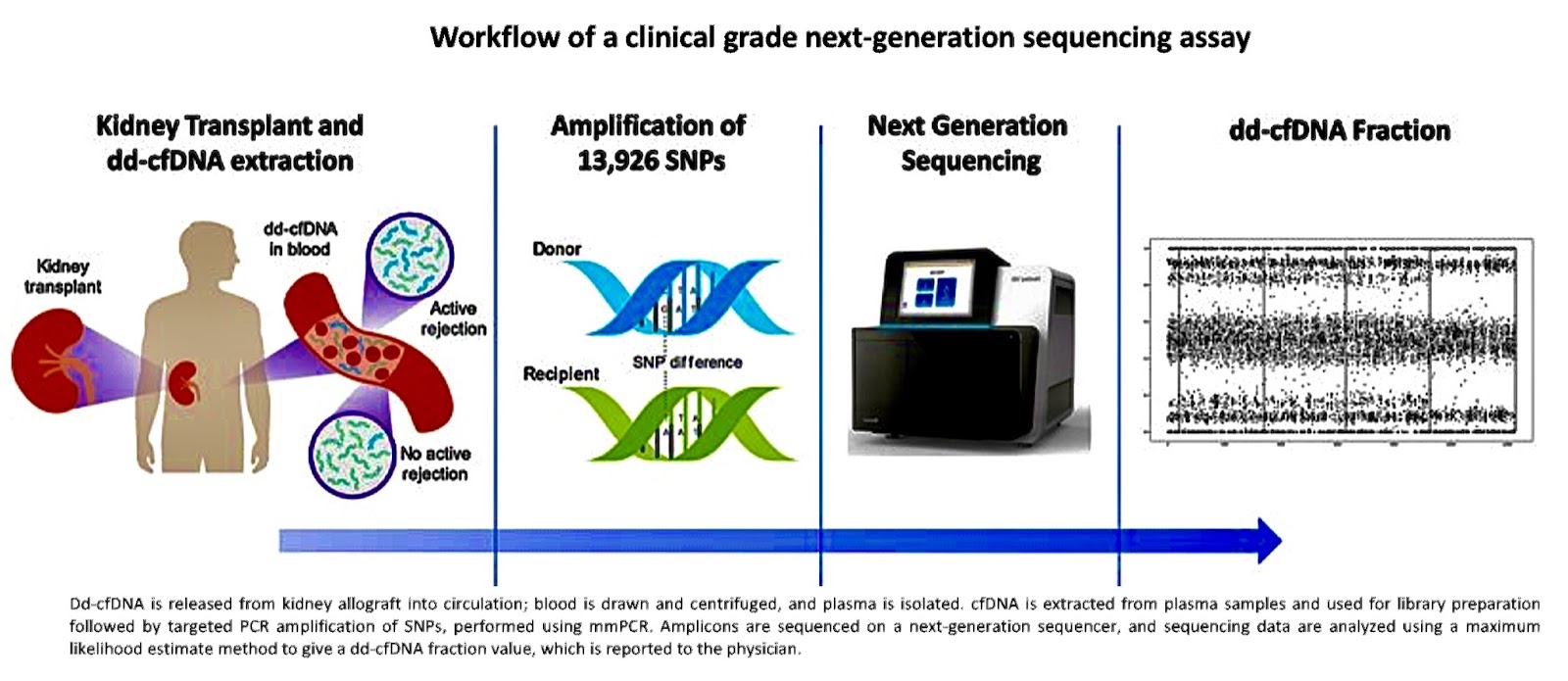
Cell free DNA are fragments of DNA that is released into the bloodstream from the cells following injury or apoptosis. Donor-derived cell-free DNA (dd-cfDNA), as the name suggests, is the DNA fragment released from injured donor allograft cells. It is measured either as an absolute value (copies/ml) or as a proportion or fraction of total cell-free DNA (%) in the recipient’s blood stream. Fractional value is simply a ratio of donor derived cfDNA to recipient derived cfDNA in percentage value.
DNA is present inside the cell nucleus wound around histones forming nucleosomes. When a cell undergoes necrosis or apoptosis, nucleosomes are released into the bloodstream where they are cleaved by nucleases resulting in approximately 120 to 170 base pair pieces of double stranded DNA. Once released, they are quickly cleared by liver, spleen and kidney with a short half-life of around 30 mins to 2 hours.
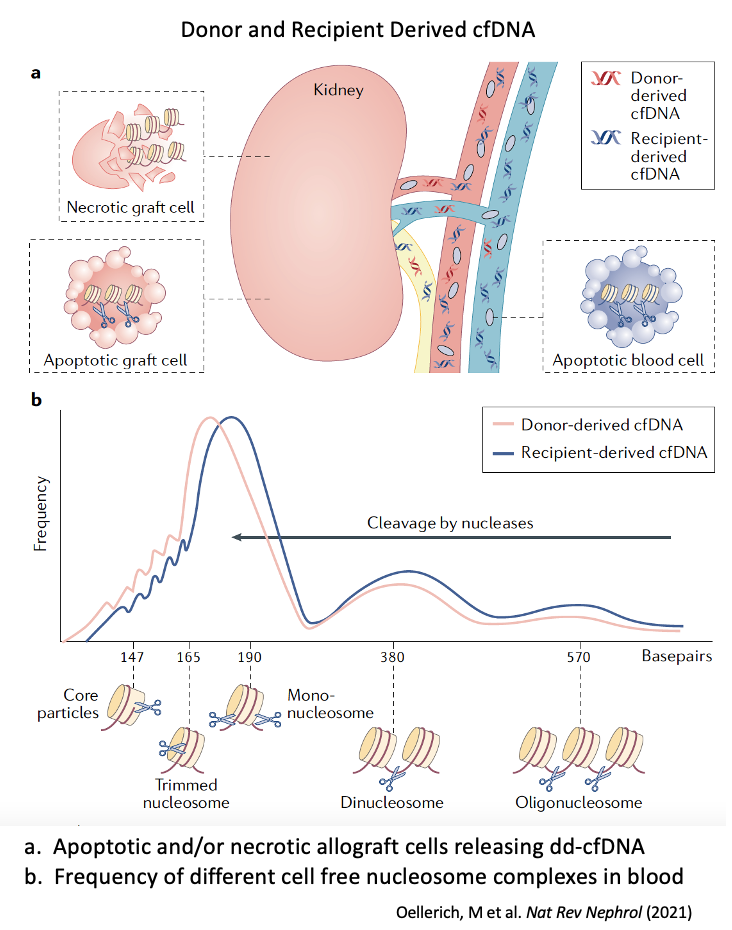
The dd-cfDNA is a very small fraction of total cfDNA fragments in the blood stream of recipients. Most of the DNA fragments (greater than 95%) in the blood are derived from the apoptosis of the recipient’s hematopoietic cells. However, during allograft injury, as in rejection, a significantly higher amount of dd-cfDNA is released in the bloodstream, thus increasing the total percentage of the donor derived cfDNA fragments. Measuring such a rise in dd-cfDNA by special assays would indicate graft injury, the commonest of which is from rejection. Median baseline value for fractional dd-cfDNA in non-rejecting, stable recipients is about 0.2 to 0.4%, while cut-off value for rejection, in most of the studies, was reported as greater than 1% (of total cell free DNA fragments in recipient’s blood).
The presence of donor specific cfDNA was first described in 1998 in plasma from female recipients of kidney transplants from male donors, using Y chromosome specific PCR. The authors concluded that donor derived cfDNA could possibly be utilized as a marker for graft cell death, and in turn, detection of kidney allograft rejection. Such differentiation was limited to sex-mismatched organ transplantation at the time. Since then, the development of targeted next generation sequence technologies using single nucleotide polymorphism (SNP) has enabled the quantification of both donor and recipient cfDNA allowing broader diagnostic applications.
Assays for dd-cfDNA
Currently, there are two distinct approaches used for assays in measurement of dd-cfDNA, which are based on either “random” or “targeted” differentiation of donor and recipient cfDNA.
- Random approaches use adapter ligation and subsequent next generation sequencing (NGS); dsDNA fragments that carry SNP markers are sequenced as they appear in plasma.
- Targeted approaches only assess SNP loci of high minor allele population frequency; and hence only a limited number of SNPs are interrogated; and donor genotyping is not required.
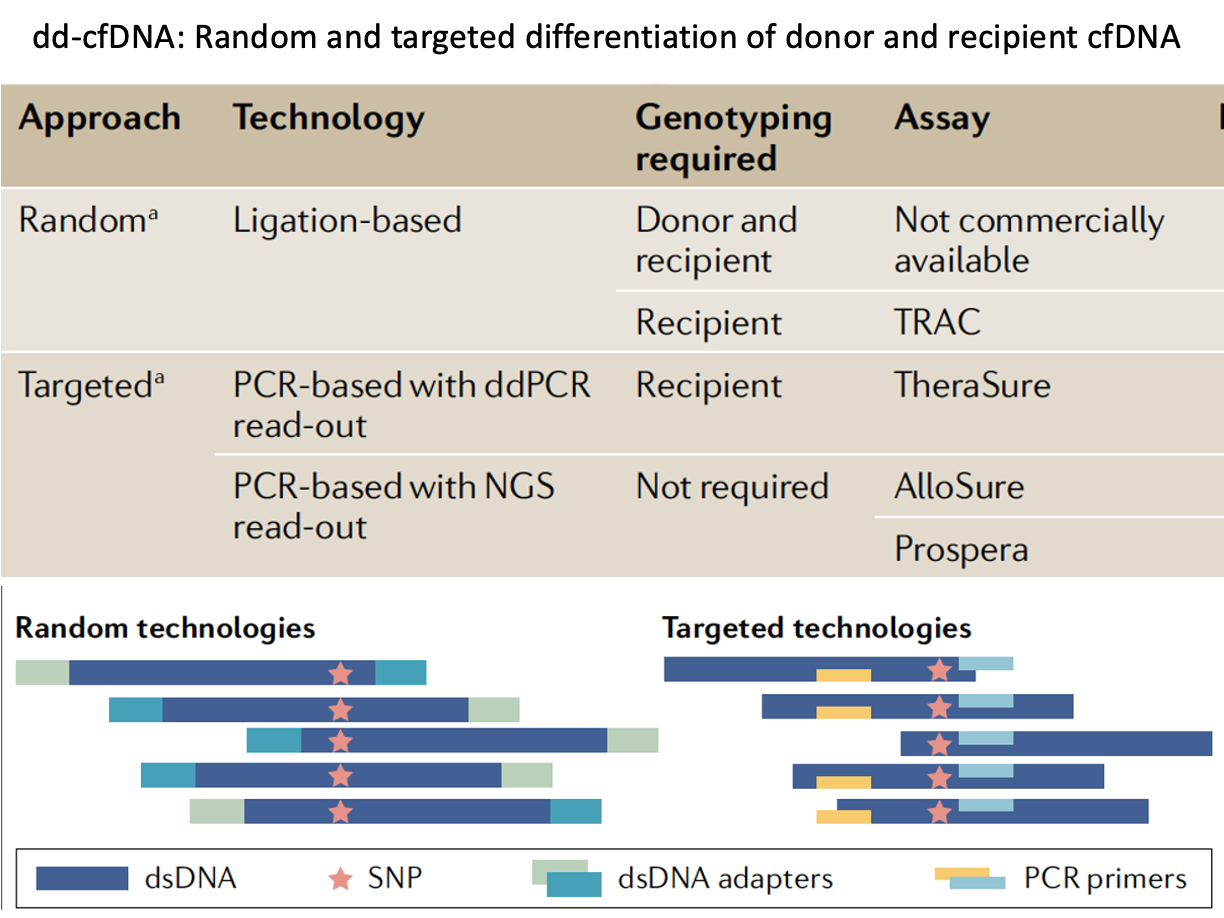
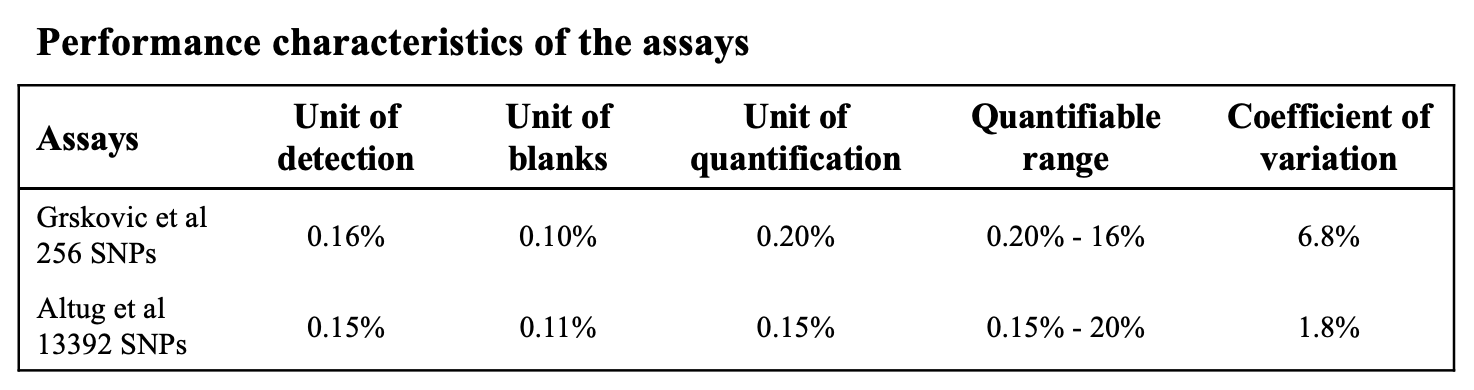
There are currently 2 commercially available tests in the United States for kidney transplant recipients- AlloSure and. Prospera. Both of which use NGS but vary in the number and specific SNPs they use in assays. The AlloSure uses 266 SNPs while the Prospera uses 13392 SNPs. Grskovic et al, developed and validated a targeted NSG assay, using 266 SNPs and reported the reliability of measuring dd-cfDNA across a linear quantifiable range (0.2% to 16%). Altug et al, using 13392 SNPs assay, reported similar results with better coefficient of variation (1.8% vs 6.8%) on repeated measurements on the same sample.
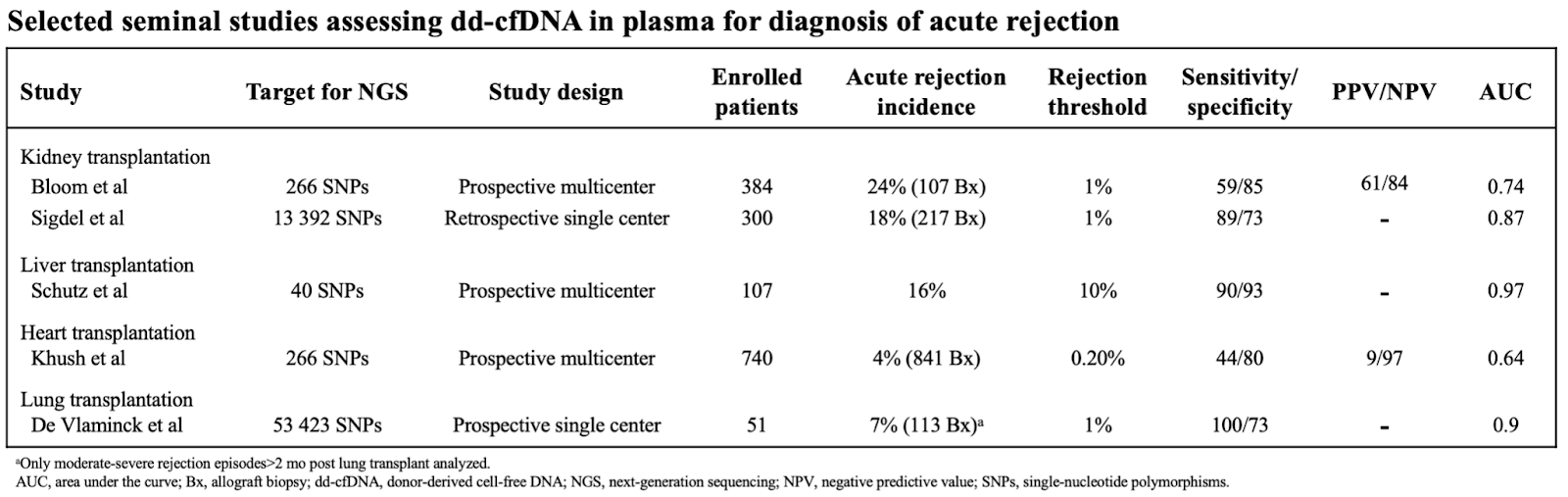
The DART study (Diagnosing Acute Rejection in Kidney Transplant Recipients) was the first to report initial results using AlloSure test in a prospective, multicenter trial to evaluate dd-cfDNA in diagnosis of acute rejection. The dd-cfDNA level with cut-off of greater than 1% discriminated biopsy specimens showing rejections and control. Sigdel et al reported the results of the Prospera test in a single-center retrospective cohort. It demonstrated AUC of 0.87 using the similar cut-off level of 1% to differentiate between rejections and controls. Seminal studies which evaluated dd-cfDNA for diagnosis of acute rejection in solid organ transplants are summarized in Table 2.
Absolute vs Fractional dd-cfDNA
Absolute dd-cfDNA is measured in copies/ml while fractional dd-cfDNA is a proportion of donor derived DNA measured as a percentage of total cfDNA in the bloodstream. Fractional determination of the cfDNA and its clinical use assumes a constant level of recipient cfDNA in blood. In other words, the denominator (recipient cfDNA) is constant and the changes in the fraction truly represents the changes in dd-cfDNA. However, damage to host cells results in release of its DNA in the bloodstream and causes spuriously low value for fractional dd-cfDNA by increasing the denominator value. These changes in host derived cfDNA levels can be caused by a variety of conditions including exercise, infection, leukocytosis, and inflammation from autoimmune diseases. This limitation may be overcome by measuring the absolute value of dd-cfDNA which can eliminate the variability of host cfDNA levels.
Whitlam et al, in a prospective study of 61 samples, compared the diagnostic accuracy of absolute vs fractional dd-cfDNA levels and showed a similar AUC for prediction of rejection. Oellierich et al, similarly, showed improved accuracy with absolute level of dd-cfDNA compared to fractional value. Another study by the same group compared the accuracy of absolute levels of dd-cfDNA during a longer period of follow-up (12 to 60 months) post-transplantation. The authors reported that absolute levels remained stable over extended periods of follow up while fractional value increased over time (due to progressive decline in host derived DNA beyond one year post transplant). The results suggested that reliance on fractional dd-cfDNA will potentially increase the false positive tests and that absolute level may be superior for long term surveillance.
Although results of fractional value are affected by variation in recipient derived DNA; compared to absolute value, it is less sensitive to pre-analytical variables such as DNA extraction efficiency and can be compared across studies. Fractional value is also not affected by rate of DNA clearance from blood stream as both donor and recipient DNA will change equally without affecting the ratio.
Dd-cfDNA in T Cell Mediated Rejection
Several studies have shown sufficient evidence that plasma dd-cfDNA is a sensitive marker for the diagnosis of rejection. However, sensitivity is known to be significantly less for T cell mediated rejection (TCMR) as compared to antibody mediated rejection (ABMR).
In the DART study, patients with early TCMR (Banff IA) had a low median value of dd-cfDNA (0.2%) which was smaller than the “no rejection” group. (0.3%). However, for TCMR (Banff IB or higher), median value was 1.2% suggesting that plasma dd-cfDNA levels with cut off value of > 1% could predict severe TCMR but not borderline or early TCMR. Huang et al, in a single center study, showed similar results. Two recent meta-analyses also reported poor diagnostic accuracy of dd-cfDNA for patients with early TCMR (Banff 1A or borderline).
Accordingly, one study, using INDEL PCR demonstrated that using smaller amplicons (86-128 bp) detected significantly higher DNA as compared to longer amplicon sizes (106-156 bp) in patients with acute rejection. Another retrospective study with a similar approach but using SNP-based multiplex PCR NGS showed higher median dd-cfDNA level with TCMR and that dd-cfDNA value did not differ significantly between AMR and TCMR patients.
In a recent multicenter study on patients with early TCMR treated with pulse steroids, authors reported significant differences in outcomes (GFR decline, development of SDA, recurrence rejection rate) between pts with dd-cfDNA >0.5% as compared to < 0.5% suggesting potential role of dd-cfDNA in further risk stratifying early TCMR when combined with Banff histology. Early TCMR histology accounts for a significant fraction of subclinical rejections (SCR). Due to apparent lack of sensitivity of dd-cfDNA in predicting such cases, further controlled studies are needed to evaluate its role in early TCMR.
Dd-cfDNA in Antibody Mediated Rejection
In patients with ABMR, multiple studies have demonstrated plasma dd-cfDNA levels to have robust predictive value for rejection. The studies have consistently reported high median values of dd-cfDNA, ranging from 1.4 to 2.9% and high predictive value with cut off > 1%. In a recent systematic meta-analysis, the composite weighted median value of DNA was 2.8% for diagnosis of AM. Both absolute and fractional values of DNA have been shown to correlate well with AMR. Presence of donor specific antibodies (DSA) improves the diagnostic prediction of dd-cfDNA for AMR. The dd-cfDNA can potentially differentiate between benign DSA and the one which results in allograft rejection. Zang et al, in a prospective study, demonstrated that dd-cfDNA discriminated between DSA positive ABMR from that of DSA negative and normal histology with AUC of 0.90 and NPV of 0.88, suggesting that negative dd-cfDNA in patients with positive DSA but without clinical manifestations can potentially avoid unnecessary biopsy. In the study, dd-cfDNA level was comparable between patients with DSA positive ABMR and sub-group of patients with positive DSA and negative histology suggesting the potential early diagnosis of ABMR with cfDNA and that biopsy may have missed the occult injury to the graft.
Dd-cfDNA in Surveillance
Most studies have shown predictable and rapid decline of plasma dd-cfDNA level with the treatment of rejection although it should not be utilized as a sole marker for resolution of active rejection as low dd-cfDNA value does not rule out ongoing rejection. The role of cfDNA in serial surveillance remains to be determined and the ideal frequency of performing the dd-cfDNA testing is still unknown. Currently, many studies are ongoing to address these very questions.
Time dependency of dd-cfDNA
The dd-cfDNA level declines exponentially to baseline value after 2 weeks post-transplant. These values are lower in the first week for living related grafts as compared to deceased donors, which might reflect increased ischemia-perfusion injury in the deceased donor setting.
The fractional dd-cfDNA level rises over the next 5 years after transplant, to a value ranging from 0.8% to 2.1% in stable conditions. Recipient cfDNA levels are high for the first year after transplant and then steadily declines to baseline values, close to that seen in healthy individuals. This time dependency of fractional dd-cfDNA levels raises the question regarding the practice of using one cut-off value for all time periods since transplantation.
Limitations
The dd-cfDNA is a non-specific marker of graft injury and not rejection-specific.
Multiple studies have shown that dd-cfDNA is not sufficiently sensitive for early TCMR and subclinical rejection. Assays for dd-cfDNA have been calibrated to histopathology, which itself is subject to interobserver variation. The assay does not discriminate patients with interstitial fibrosis and tubular atrophy (IFTA). The use of one cut-off value for predicting rejection over varying time period post transplantation remains questionable owing to the time dependency of host cfDNA. Underestimation of dd-cfDNA using PCR-based methods is unavoidable with current methodological limitations. Further studies are needed to evaluate uncertain economic implications of routine testing.
Conclusion
Overall, there has been adequate evidence to suggest favorable potential of dd-cfDNA in detection of graft rejection at an early stage. Further prospective, randomized trials will be required to investigate the role of dd-cfDNA in improving outcomes. Currently, there is no sufficient data to recommend using dd-cfDNA levels for continuous, long-term surveillance. Combination of dd-cfDNA with existing parameters and other novel markers like chemokines, microRNAs should be further explored. Given the limitations, dd-cfDNA should be interpreted only in combination with all available relevant clinical data and other diagnostic findings
Reviewed by Matthew A. Sparks, Sam Kant