Laura Slattery, Specialist Registrar in Nephrology and General Internal Medicine, Royal College of Physicians, Dublin.
Paracetamol or acetaminophen ingestion can result in a variety of toxic syndromes predominantly related to alterations of glutathione metabolism and/or depletion of glutathione stores. Acute overdose can result in hepatic toxicity, and in some instances- fulminant hepatic failure.
When we are confronted with consults about toxidromes on the nephrology consult service, acetaminophen toxicity is not the first thing that springs to our minds. Perhaps this undoubtedly underdiagnosed clinical entity should be. Increasingly, there are case reports and case series describing the development of high anion gap metabolic acidosis (HAGMA) following acetaminophen exposure and subsequent detection of 5-oxoproline in blood or urine.
Case discussion
“Can you review this patient? Her respiratory rate has increased and she is more drowsy. Her blood gas is very abnormal and we would appreciate some advice”
This was the consult call for a 70-year-old woman admitted under a surgical team following a complex orthopaedic history. The initial presentation was with a left intertrochanteric fracture following a fall and subsequent left hemiarthroplasty. She was discharged to rehabilitation in the post-operative period, however she subsequently was readmitted six weeks later with suspected infected prosthesis culminating in revision total hip replacement and washout- cultures yielded a methicillin sensitive Staphylococcus aureus from OR samples and admission peripheral blood cultures.
Past medical history of note included COPD (60 pack year smoking history), atrial fibrillation (on warfarin), osteoporosis, low BMI, and a prolonged history of alcohol excess up right up to the time of admission.
Review of her medications- Warfarin as per INR, bisoprolol 5mg, furosemide 20 mg, atorvastatin 10 mg and ipratropium bromide inhaler. Since admission, she had been on IV flucloxacillin 2 g four times daily, acetaminophen 1g four times daily and had received 5 L normal saline with the justification of “poor intake”
This clinical deterioration occurred on day 10 of her admission. On review, Glasgow Coma Scale was 13/15 (E3V4M6), she was tachypneic at 25 breaths/minute, oxygen saturations 92% on room air. Other vital signs were within physiologic range. Portable chest X-ray: Mild cardiomegaly with no signs of infection or congestion. Urgent laboratory testing was performed.
| ABG | Biochemistry |
| pH 7.2 | Na+ 146 mmol/L |
| pCO2 3 kPa (23 mmHg) | K+ 3.2 mmol/L |
| pO2 11.7 kPa (88 mmHg) | Cl– 118 mmol/L |
| Bicarbonate 8 mmol/L | Creatinine 140 umol/L (1.6 mg/dl) |
| Lactate 1.8 | Albumin 22 g/L(2.2g/dL) |
Working through these results, the anion gap corrected for albumin: 25 mmol/L, with delta-delta ratio of 0.8. The expected pCO2 by Winters formula: 2.5-3 kPa leading to a diagnosis of “pure” high anion gap metabolic acidosis. Here is an excellent NephSIM post for working through acid base problems using the PLACO mnemonic; pH, Labs, Anion Gap, Compensation, Other.
Working through the “GOLDMARK” mnemonic led us to a diagnosis of 5 oxoprolinaemia.
- Glycols (ethylene glycol, propylene glycol) hospitalised inpatient with no access to these so unlikely
- L-Lactate (standard lactic acid seen in lactic acidosis) Lactate 1.8
- D-Lactate (exogenous lactic acid produced by gut bacteria)
- Methanol Hospitalised inpatient with no access to these
- Aspirin (salicylic acid) Level <0.1
- Renal Failure (uremia) urea 10
- Ketones (diabetic, alcoholic and starvation ketosis) glucose 5 ketones 1
Acetaminophen was immediately discontinued, flucloxacillin was changed to ceftriaxone (reasons for change discussed below). N-acetylcysteine commenced and she received isotonic sodium bicarbonate x 2 followed by oral sodium bicarbonate 1.2 g TDS. Unfortunately, she continued to deteriorate with persistent acidemia, low GCS, and ultimately cardiorespiratory failure and death some two days later. Approximately 2 weeks later her urinary 5-oxoproline concentration results returned at 10 mmol/mmol creatinine (ref < 0.1).
Discussion
Metabolic acidosis that is caused by 5-oxoproline results from disruption of the γ-glutamyl cycle. Inherited forms of enzyme defects have been implicated in the overproduction of 5-oxoproline described including glutathione synthetase deficiency and 5-oxoprolinase deficiency, both of which result in massive urinary excretion of 5-oxoproline. The syndrome of acquired 5-oxoproline (pyroglutamic acid) metabolic acidosis with described in 1989: Creer et al. reported a 52-year-old woman with anion gap metabolic acidosis caused by systemic accumulation of 5-oxoproline (a strong organic acid; pKa=3.6) and 5-oxoprolinuria. Accumulation of 5-oxoproline results in subsequent development of anion gap acidosis. Of note, 5 oxoprolinaemia is a distinct entity from acute acetaminophen toxicity. Additionally, Acetaminophen levels are very rarely in the toxic range and cases do not usually have other indicators of acetaminophen toxicity such as elevated hepatic transaminases or prolonged prothrombin time.
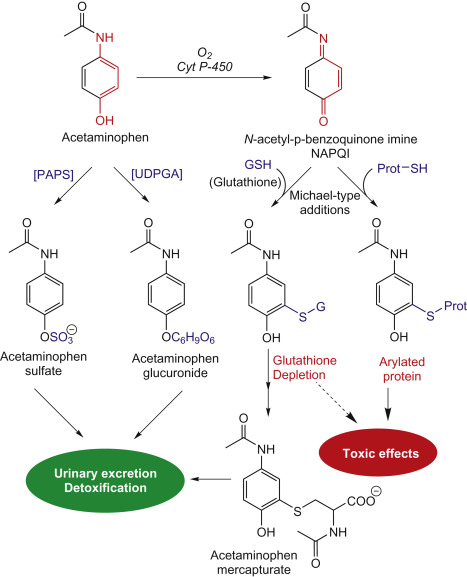
Acetaminophen is hepatically metabolized and subsequently excreted into the urine: approximately 50% as glucuronide acetaminophen conjugates, 40% as sulphated acetaminophen conjugates and 5% unchanged. The remaining 5% is oxidised by cytochrome enzymes to produce N-acetyl-p-benzoquinoneimine (NAPQI) which is a highly reactive oxidation product. NAPQI is ultimately detoxified by glutathione and nontoxic metabolites are excreted in the urine.
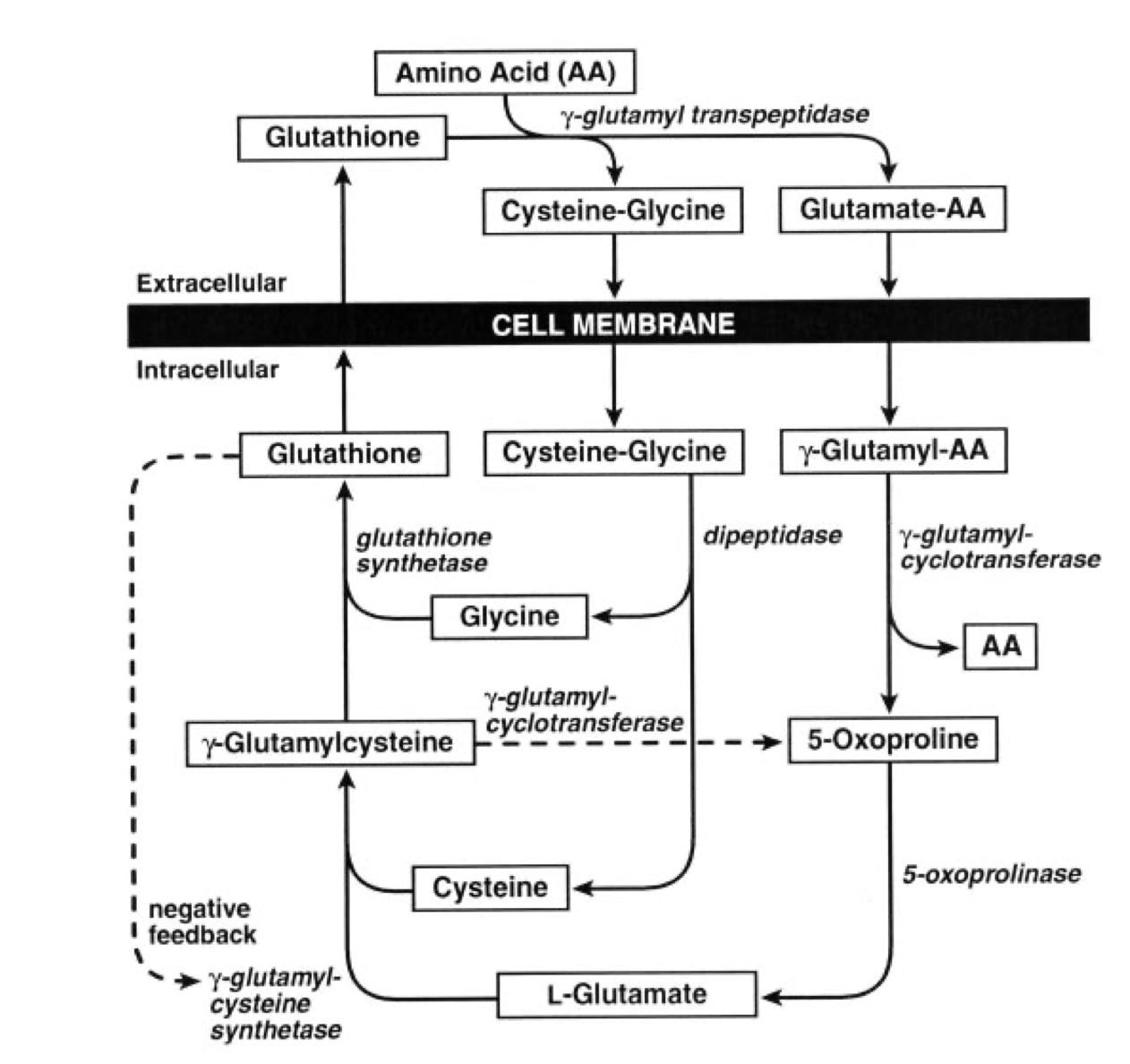
In the gamma-glutamyl pathway, 5-oxoproline is an intermediate and is responsible for generating glutathione. As demonstrated below, normal glutathione stores are required for feedback suppression of the enzyme gamma-glutamylcysteine synthetase which is the gate-keeper for the cycle. Chronic or subacute injection of acetaminophen depletes glutathione stores primarily through metabolism of acetaminophen to NAPQI, leading to repeated depletion of glutathione stores. This ultimately results in loss of feedback inhibition and increased production of 5-oxoproline from its precursor gamma glutamylcysteine. 5-oxoprolinase usually degrades 5-oxoproline; inhibition of this enzyme by flucloxacillin can also promote 5-oxoproline accumulation as with our patient.
Risk factors that predispose to development of the condition include female sex (preferentially metabolise acetaminophen to sulfated derivatives) malnutrition, sepsis, diabetes, underlying liver disease and pregnancy. Chronic acetaminophen ingestion likely also consumes glutathione stores and predisposes to development of the disorder. Impaired kidney function has also been independently identified as a risk factor due to decreased clearance of 5 oxoproline.
Many cases go unrecognised until the clinical syndrome is at quite an advanced stage due to both a lack of awareness, but additionally because the assay for 5 oxoproline is not widely available. Therefore, making the diagnosis is challenging and requires a high index of suspicion.
Furthermore, management is challenging, particularly given cases are often at the severe end of the spectrum once recognised. Management involves urgent review of medications; Discontinuation of medications that can inhibit enzymes involved in the γ-glutamyl cycle and that consume glutathione, aggressive treatment of associated risk factors such as malnutrition and supportive management. Intuitively, repletion of glutathione stores represents a possible therapeutic moiety in the form of N-acetylcysteine; the “antidote” for acetaminophen toxicity; although there are case reports supporting this, there is no definitive evidence to back its use. Isotonic bicarbonate therapy may also be considered; again this is supported by case reports only. The compound is not known to be cleared by any haemodialysis modality.
In conclusion, this is a rare though probably underdiagnosed cause of metabolic acidosis with increased anion gap. The disorder of 5-oxoprolinemia should be considered in patients with unexplained HAGMA; particularly those with chronic or subacute acetaminophen use combined with malnutrition, sepsis. Awareness and the maintenance of a high index of suspicion are imperative for recognition and institution of management strategies
Reviewed by Sam Kant, Matthew A. Sparks and Josh King.
With the move to minimize opioids post-operatively (which is a good thing), I see this every now and then.
@HumphreysLab gets a hat tip for pointing this out a long time ago.