Mythri Shankar, MD, DNB
Assistant Professor of Nephrology
Institute of Nephrourology, Bengaluru, India
@nephromythri
Yuri Gagarin was the first human to leave earth in the year 1961. Since then over 500 astronauts and cosmonauts have visited space. During the initial days, the duration of space flight was short. The maximum duration in 1970 was only 18 days, but this was actually an endurance record. It was difficult to sustain for longer periods of time due to a shortage of food supply as there was less space for carrying supplies in small sized spacecraft and other technical constraints such as lack of medical monitoring of the crew members and so on.
To overcome this barrier, from the 1970s through 1980s a series of experiments were performed to build international space stations by Russia and the United States. These space stations helped in extending the duration of stay in space and conduct experiments to study adaptation and changes in human physiology due to longer duration of stay in space.These experiments and research are important to explore the possibilities of “living in space” concept like living on Mars or Moon.
The first experimental space station was the Russian salyut station in 1971. This was followed by a number of other space stations such as Skylab 1, Salyut 6, Salyut 7 and Mir that supported the astronauts and cosmonauts for longer duration stay extending to over 200 days before the International Space Station was formed.Today, astronauts from all around the world visit International space station which serves as space environment and microgravity research lab.
Astronauts and cosmonauts are exposed to microgravity in space. Body fluid regulation is completely different in microgravity compared to the earth.The fluids in the body are pulled down by gravity and they return back to the heart by the activity of muscles. However, in space, due to lack of gravity, fluid accumulates around the head and the chest. This fluid accumulation results in baroreceptor activation and pressure natriuresis. Thus, the body’s natural mechanism to defend against volume overload is falsely triggered. A variety of experimental models of central hypervolemia are performed on earth to simulate this phenomenon.
- head down- tilt experiments
- acute assumption of supine position
- water immersion to the neck
- acute isotonic saline infusion.
These are the usual hypervolemia models to study human (patho)physiology. These stimuli cause natriuretic and diuretic response.The atrial-renal reflex was first explained by Henry and Gauer in 1963. They attributed the atrial-renal reflex to vasopressin and neural regulation. Today we know that there are a number of other factors contributing to this mechanism of volume loss occurring in space as a result of fluid accumulation in the head and neck due to microgravity.
A 56-day skylab mission was conducted to study the hormonal, fluid and electrolyte occurring due to extended stay in space in the 3 crew members of Skylab 3 who served as their own controls. The results showed a negative fluid balance in these three astronauts studied which was attributed to both increased evaporative loss and urinary loss of volume. The same authors also concluded that there was negative sodium balance although overall net cumulative body sodium content had increased.
For many years, the assessment of pre-flight and post-return weight of the astronauts has demonstrated that there is weight loss at the time of return to earth. This was earlier thought to be due to negative water balance due to increased urinary water loss. A report from voluntary dietary intake of astronauts on life and microgravity sciences (LMS) shuttle mission and also data from US – mir shuttle mission (mir is the name of a Russian space station, US-mir shuttle mission was a collaboration between US and Russia to form the present International Space station) confirm that most of the astronauts have a reduced dietary intake similar to a state of dormancy. Another report also suggested that in long term flights (more than a few months) , muscle loss significantly contributed to weight loss apart from body fluid loss.
Microneurography is the study of peripheral nerve traffic in awake individuals. Such as the sensation of touch, pain and also constriction status of peripheral blood vessels due to sympathetic nerves supplying these blood vessels. Neurolab was a NASA space mission dedicated to study the nervous system with multinational collaboration.The primary aim of neurolab mission was to study how the nervous system adapts, grows and responds to microgravity. Plasma samples and microneurographic images from this Neurolab mission have shown considerable activation of the adrenergic system in astronauts. Persistent increase in vasopressin levels despite motion sickness was observed. Vasopressin is considered to be the etiologic hormone for motion sickness, however its causal role has been controversial. Activation of renin aldosterone system was seen in the Euro’MIR94 mission and Spacelab D-2 mission
So theoretically, loss of fluids should cause hypotension but there is activation of the adrenergic system. So are astronauts prone for hypertension? Can volume depletion cause paradoxical hypertension? Am I making an astonishing statement here? Let’s find out!
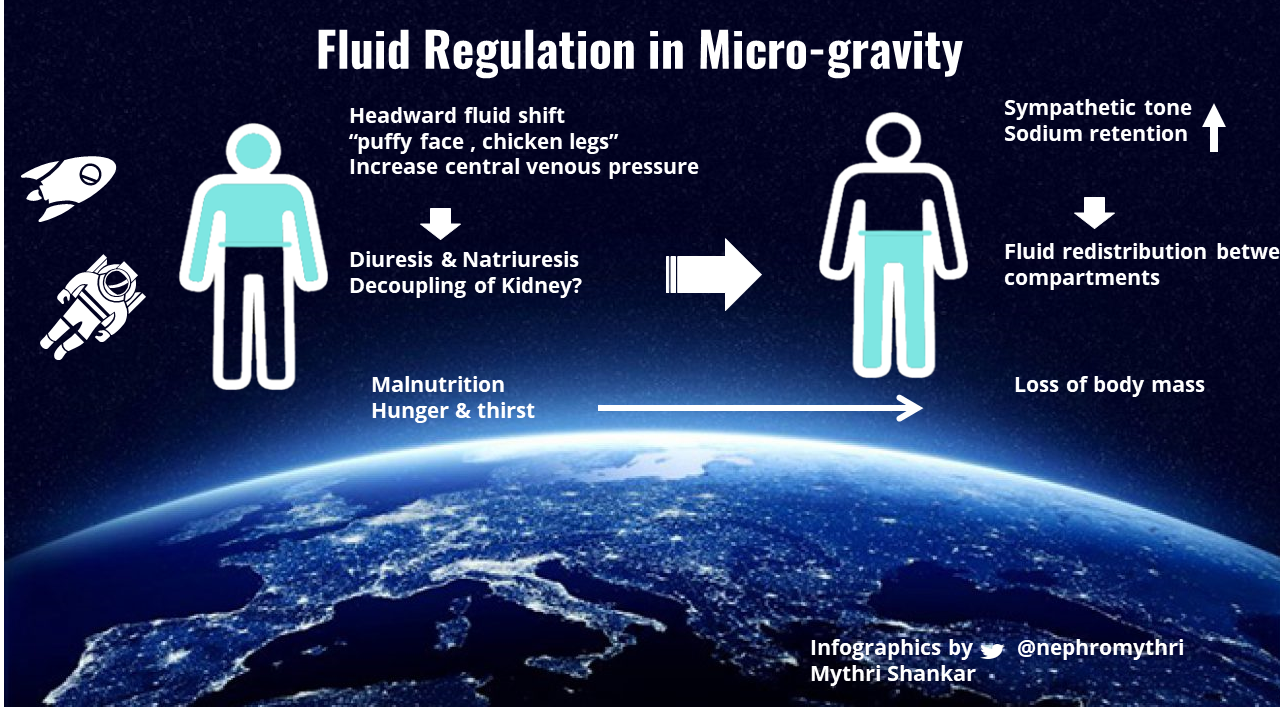
Image 1: Adaptation of human fluid balance in microgravity
In order to understand this, we will have to know the meaning of the term “aestivation”.
All organisms are propelled by “self-centered” genes which motivate them to live, grow and reproduce.The three main ingredients for life are
- water (solvent of life)
- nutrients (building blocks of life)
- energy (ATP produced from oxidative respiration).
When there is shortage of one of these three ingredients, the organism goes into dormancy which is a state of hypometabolism in order to prevent death. This is called “aestivation”. It is derived from the Latin word “Aestas” which means summer. Aestivation is typically defined as dry season dormancy. Arid conditions with restricted food and water supply are the main drivers of aestivation.
The biochemical and physiological aspects of aestivation are well researched in animals like lungfish (Protopterus sp), land snails (Helix Sp) and water holding toads (Cyclorana sp). The paramount features of aestivation are
- strategies to store body water
- hypo-metabolic state
- energy conservation
- altered nitrogen metabolism
- mechanisms to stabilize cells in dormant state.
Cell- signaling pathways like those mediated by FoxO1, ERK, Akt, AMP-activated kinase play an important role in aestivation.
You must be wondering here as to what has aestivation got to do with astronauts?
Let me explain. There is fluid loss happening in the astronauts as discussed already. Also, due to limited availability of food and water resources in space, they are pushed to a state of starvation. Our wonderful human body senses this and adapts to survive by switching on the “aestivation mode”.
Recently, two animal models have been studied to look into the physiological and biochemical adaptations secondary to experimentally induced water loss in rats
Firstly, Kovarik et al studied Sprague Dawley rats by surgically resecting ⅚ kidney mass (surgical kidney disease) and inducing chronic kidney failure.
Kidney Water loss:
The investigators studied the urine concentration of rats with surgical kidney disease and found that there was 50% reduction in urine osmolality and urine free water excretion was increased by 33.9 ml/kg/day. Predominant osmolytes in the urine were urea, followed by K+ and Na+ with their accompanying anions. They also found an increase in plasma osmolality predominantly due to an increase in urea (79%) followed by K+ (20%) compared to the controls. Hence, it was concluded that surgical kidney disease caused urine concentrating defects leading to polyuria and kidney water loss.
This kidney water loss initiated an aestivation state in these rats leading to increased production of urea by the liver. This increased urea levels in turn increased the plasma osmolality, in order to hold on to the body water content.
Urea is a breakdown product of protein metabolism. However, it was observed that both rats with surgical kidney disease and control rats had similar food (protein) intake patterns. Ever wondered how the liver manages to produce excess urea? What is the source of nitrogen for this excessive urea production? The investigators noted that rats with surgical kidney disease used their muscle branched chain amino acids and anserine and carnosine stores (metabolic energy and nitrogen reservoirs of the muscle) to generate more urea by the liver in order to hold on to the body water content. Hence, rats with surgical kidney disease exploited endogenous muscle protein stores and fat stores to produce urea and other osmolytes.
Another interesting finding was the steady increase in blood pressure in rats with surgical kidney disease despite kidney free water loss. This was accompanied by peripheral vasoconstriction. Four mechanisms were postulated for this phenomenon :
- Increased production of NO synthase inhibitors
- Increased free radical injury to the endothelium
- Increased production of copeptins (by product of vasopressin)
- Increased sympathetic nerve tone (increased urine norepinephrine levels)
So, do rats with surgical kidney disease constrict their cutaneous vessels in order to reduce transepidermal water loss (TEWL) as a part of the water conservation process? Does this peripheral vasoconstriction increase the afterload and hence the arterial blood pressure? In order to explore the possible answers to these questions, the investigators performed another experiment.
They exposed rats with surgical kidney disease to higher temperature of 36.5 degree celsius as opposed to 33 degree ambient room temperature, which caused peripheral vasodilation to dissipate heat and hence drop in blood pressure. Now the blood pressure was similar to that of the control rats. Thus, supporting their hypothesis that rats with surgical kidney disease constricted their dermal vessels as a physiological adaptation to conserve water which was lost in the urine.
All these observations point to the possibility that hypertension could be a side effect of the body’s successful mechanism to conserve water in a state of dehydration.
Here is the second animal experiment. Wild et al studied a mouse model by inducing psoriasis by transgenic overexpression of IL-17 in keratinocytes. Due to the defective epidermal barrier there was increased transepidermal water loss. This water loss was similar to that caused by surgical kidney disease in Sprague Dawley rats. The aim was to study the body’s adaptation to water loss. As an adaptive mechanism, in areas where the epidermis was intact, there was severe cutaneous vasoconstriction to prevent water loss, reduced kidney water loss and highly concentrated urine. Accordingly, water intake was increased. The investigators noticed an increase in urea transporter A1, aquaporin and the transcription factor TonEBP (Tonicity enhancer binding protein) in the kidney medulla as well as in the skin. This shows the adaptation to conserve water by increasing reabsorption of urea and water in the kidney medulla and the skin. Also, other compensatory mechanisms to increase plasma osmolality. Weight analysis showed a reduced dry weight and increase in water to tissue ratio in psoriatic mice compared to the wild type. This was due to exploitation of endogenous muscle mass to synthesize urea and organic solutes.
Also, the liver mass was increased by 50% in psoriatic mice compared to the wild type. Liver is the site for synthesis of urea and other organic solutes.
At 36 degree celsius (normal body temperature) skin blood flow to the hind paws was lower compared to the wild type. But as temperature increased to 40 degree celsius, there was vasodilation and blood flow was similar to the wild type. However at this high temperature, the blood pressure of psoriatic rats dropped to normal levels. This re-emphasises the observation that hypertension is due to physiological adaptive peripheral vasoconstriction for water conservation when an organism is prone for dehydration stress.
This mechanism has been well described in Homer Smith’s “Fish to philosopher” book, where organisms evolved from fish to amphibians and later into mammals which survived in arid land. Hence, physiological adaptation to water shortage – aestivation, has been an evolutionary survival strategy. When amphibians moved to brackish waters (salty waters but not as salty as the sea), they were exposed to a high saline environment leading to dehydration. In order to avoid dehydration, aestivation mechanisms produced more solutes to retain body water content. They reduced dermal and kidney excretion of urea and increased the levels of urea in their skin and body tissues.
Studies in lung fish or cartilaginous fish, has shown that it is predominantly urea and endogenous organic osmolytes production which is contributing to the overall high blood osmolality compared to ions like Na+ , K+. This is because urea and other organic osmolytes can be produced from endogenous protein (muscle) breakdown, whereas for ions like Na+ and K+, the aestivating organism has to depend on the environment. Also, urea readily moves from intracellular to extracellular compartment and vice-a-versa in order to maintain equilibrium.
Hence, this evolutionary adaptive mechanism – aestivation explains the reasons for sarcopenia and hypertension in kidney failure and other conditions of water loss.
These two animal models (surgical kidney disease and psoriasis) provide novel pathogenetic concepts for the cause of hypertension. Aestivation and peripheral vasoconstriction as the reason for hypertension is a simple mechanism to explain. This however does not invalidate pressure natriuresis theory.
We have noticed that our aging population has essential hypertension along with loss of body mass. Skin is the largest organ in the body. These two studies encourage researchers to look into therapeutic options aimed at preventing dermal vasoconstriction to treat hypertension.
On recalling the results of the studies conducted in the space lab and the mice lab appear similar. There is loss of body fluid and body mass in both. Also both had increased sympathetic hormones in circulation. This also calls for more research in the field of body fluid mechanics in microgravity compared to Earth.
Reviewed by Matthew A. Sparks and Amy Yau

